Autonomous Medical Coding in 2026: Accuracy, Denials, Payer Rules & ROI
Discover how autonomous medical coding works, how it differs from CAC, and how it helps boost accuracy, reduce denials, and support RCM teams.
Published on:
November 18, 2025
Updated on:
July 27, 2026


Key Takeaways:
• Autonomous medical coding uses advanced AI to read clinical documentation, apply coding guidelines, and generate complete, compliant code sets—while knowing when to escalate uncertain cases to humans.
• Unlike CAC, which only suggests codes, autonomous systems complete the entire workflow for high-confidence charts and act as a scalable “junior coder” that reduces workload and bottlenecks.
• Autonomous coding became possible through breakthroughs in PLM-ICD models, large language models, retrieval-augmented reasoning, and multi-agent architectures with built-in explainability.
• Autonomous systems significantly reduce denials, boost accuracy, ease coder shortages, and cut administrative costs.
• CombineHealth's autonomous medical coding platform, Amy, is proven to autonomously code ~80% of charts at 98.4% accuracy, being payer-aware, and cut coding-related denials 75% while lifting captured revenue 4% in one hospital deployment.
Medical coding is a lot like translating a story for an audience that speaks an entirely different language. When a patient comes in, the provider writes the notes, but coders turn that encounter into precise numbers and letters that insurers understand. And doing that well takes far more than familiarity with ICD-10 or CPT.
That’s because coding guidelines shift every year. Payer rules don’t match each other. And every specialty speaks its own dialect—dermatology coding relies on lesion counts and sizes, while cardiology coding hinges on device placement and catheterization details.
Even the best coders are up against rising volumes, tighter turnaround times, and constant regulatory updates.
This is where autonomous medical coding technology comes in—not to replace human coders, but to extend their abilities.
.webp)
What Is Autonomous Medical Coding?
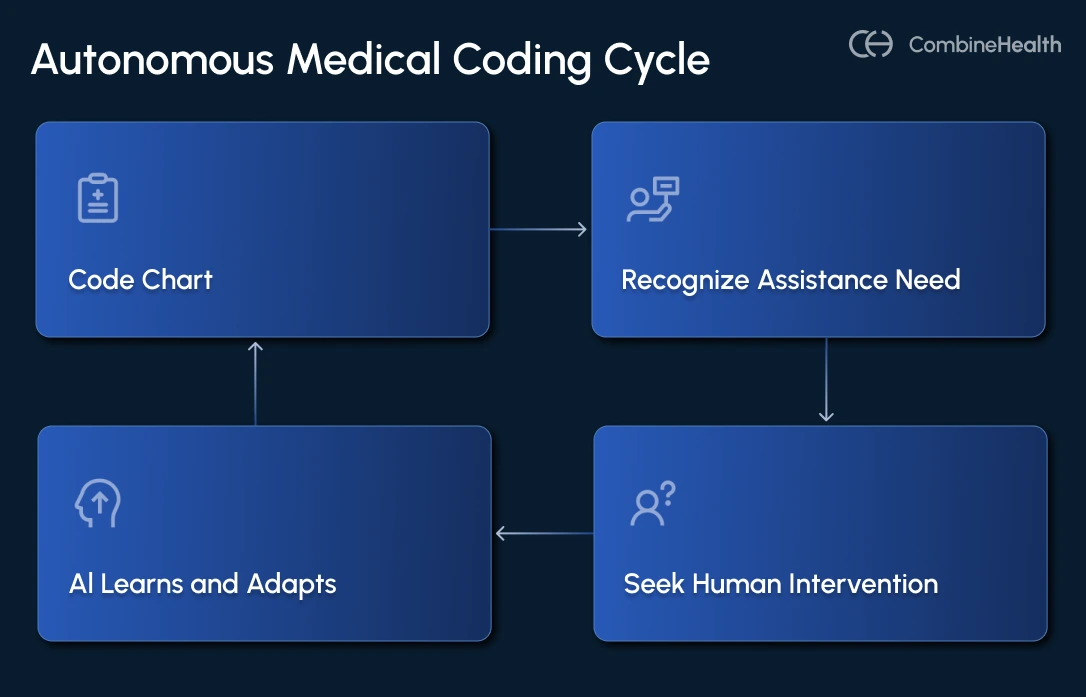
Autonomous medical coding is when AI can fully code a chart on its own, while still knowing when it needs help.
It uses advanced AI systems that can read clinical documentation, interpret the clinical story, apply coding guidelines, and generate complete, compliant ICD-10, CPT, and modifier codes without requiring a human to manually review every chart.
How Is Autonomous Medical Coding Different From Computer-Assisted Coding?
Unlike traditional computer-assisted coding (CAC), which only suggests codes, autonomous systems complete the coding workflow end-to-end for high-confidence encounters and escalate only the exceptions to human coders.
In most organizations, coders end up spending just as much time reviewing CAC output as they do coding from scratch. The software accelerates lookups, but the cognitive load and responsibility remain with the coder.
Autonomous medical coding flips that dynamic.
Think of it as a junior coder that can finish entire encounters on its own. The system reads the full chart, assembles a complete, compliant code set, performs its own internal checks, and only sends cases to humans when something is unclear or inherently risky.
Recommended Read: How AI is used in healthcare RCM
How Does Autonomous Coding Work?
Autonomous medical coding solutions use a coordinated stack of NLP, machine learning, transformer models, and clinical knowledge engines to read provider documentation and assign the correct ICD-10 codes, CPT codes, E/M codes, and modifier codes.
Here’s a step-by-step breakdown of how the process works:
1. Data Ingestion
The system connects directly to the EHR and pulls in everything documented during the encounter—structured data (med lists, vitals, problem lists) and unstructured text (provider notes, operative reports, consults, discharge summaries).
CombineHealth’s Amy (Autonomous Medical Coding Platform) integrates directly with many EHR systems and reads all the medical data to generate medical codes.
2. Clinical Language Understanding
Advanced NLP models parse the note to identify diagnoses, symptoms, procedures, laterality, acuity, and clinical relationships.
Then, transformer-based models like ClinicalBERT or domain-specific LLMs allow the system to understand context. For example, knowing that “patient discharged home” and “purulent wound discharge” mean completely different things.
3. Code Selection
The system maps extracted concepts to ICD-10 and CPT codes using hierarchical search, guideline retrieval, and historical pattern matching. It assembles complete code sets when multiple diagnoses or procedures are required and applies the correct modifiers automatically.
CombineHealth’s Amy (AI Medical Coding Platform) supports multiple coding conventions such as ICD-10, CPT-10, E/M codes, facility codes, and HCPCS codes. She finds the appropriate codes, along with clear explanations (her thought process) on why she picked that code.
4. Compliance & Confidence Checks
Before finalizing the codes, the engine checks medical necessity, bundling rules, payer-specific edits, and documentation sufficiency. High-confidence encounters are auto-coded; lower-confidence ones are routed to human coders with explanations, evidence highlights, and suggested corrections.
To determine the MDM complexity of a case, CombineHealth’s Amy (AI Medical Coding Platform) lists down all the problems being addressed and all the data points being analyzed, along with the risk of complications.
5. Continuous Learning
Every correction from human coders, every denial, and every updated guideline feeds back into the model, ensuring the system becomes more accurate over time.
How Is Autonomous Coding Accuracy Actually Measured?
Coding accuracy is best measured at the claim-line level — each CPT code plus the ICD codes that justify it — not across the whole claim. Payers adjudicate one line at a time, so a claim with one bad line out of ten (90%) is very different from one bad line out of three (67%).
CPT code accuracy is determined by comparing the assigned CPT code against the correct code identified through expert review of the complete clinical documentation. Reviewers evaluate the chart using the latest coding standards and verify that the selected code accurately represents the service provided.
It typically involves validating the assigned code against:
- Complete clinical documentation (physician notes, procedures, test results)
- AMA CPT coding guidelines
- Specialty-specific coding guidance
- NCCI edits
- Payer-specific coding policies, where applicable
How Is ICD-10 Coding Accuracy Determined?
ICD-10 coding accuracy is measured across these five dimensions:
Is 95% Coding Accuracy Good Enough?
It depends what's being measured. A claim-level number hides line-level errors; ask any medical coding vendor how they calculate medical coding accuracy before comparing.
Amy reports claim-line metrics — roughly 97% ICD accuracy, 98% primary-diagnosis accuracy, ~98% E&M, ~97% CPT.
Why Accurate Coding Alone Isn’t Enough?
A claim can be coded perfectly and still be denied or underpaid if documentation doesn't support it. In CMS's FY2025 Medicare Fee-for-Service review, incorrect coding drove just 11.1% of improper payments, while insufficient/missing documentation accounted for about 65% and medical necessity another 15.3%.
Autonomous coding has to do more than assign codes — it must capture the care completely, strengthen supporting documentation, and apply payer requirements before the claim goes out. That's where CDI, done during coding, finds missed diagnoses, improves specificity, and surfaces supported revenue opportunities.
Case Study: Autonomous Coding + CDI Capabilities = 75% Less Denials!
At a 400-bed Midwest hospital, Amy, CombineHealth’s autonomous medical coding platform, identified undercoding that had gone undetected and, within three months, reduced coding-related denials by 75% and improved captured revenue by 4% while maintaining 98.4% accuracy — by orchestrating payer-specific policies and surfacing higher-specificity documentation.
Additionally, Amy surfaced 5× more CDI opportunities than the manual workflow.
Should Autonomous Coding Adapt to Payer Rules?
Yes, an autonomous medical coding service should be payer-aware to actually drive downstream results in healthcare RCM.
Payer-aware autonomous coding applies each payer's rules — LCDs, NCDs, specialty guidelines, and billing edits — before the claim is generated, and learns from real payer outcomes (denials, underpayments, edits) over time. That's what prevents downcoding and medical-necessity denials on codes that are technically correct.
It's also how a system keeps up with constantly changing policies: rather than relying only on static guidelines, it treats claim outcomes as feedback.
Amy applies current payer guidelines (LCDs, NCDs, specialty and payer-specific billing rules) before claim generation, and is payer-outcome-aware — reimbursements, denials, and edits feed back into future coding decisions.
How Autonomous Medical Coding Benefits Revenue Cycle Teams
Autonomous medical coding directly strengthens the revenue cycle by eliminating the bottlenecks that slow teams down. Here’s how it creates meaningful impact across coding, billing, and operations:
- Eliminates Routine Manual Work: Autonomous coding systems can process large volumes of patient charts with zero human intervention, reducing the need for manual coding and human review.
- Improves Accuracy and Consistency: Because autonomous coders apply the same rules, logic, and guidelines every time, they significantly reduce variation in coding quality. This leads to fewer missed codes, fewer compliance risks, and far fewer downstream denials caused by documentation or coding errors.
- Eases the Pressure of Coder Shortages: With medical coder turnover at historic highs, many RCM teams are stretched thin. Autonomous coding absorbs large portions of the workload, giving organizations a scalable way to handle rising chart volumes without scrambling to hire or train more staff.
- Cuts Administrative Costs and Boosts Efficiency: By reducing manual coding hours, organizations lower labor costs and minimize reliance on outsourced coding.
Should Medical Coding Be Completely Autonomous?
No, medical coding should not be completely autonomous, but AI should play a central role in a carefully designed hybrid model with strategic human oversight.
Here’s why:
1. Legal and Financial Liability Risks
The legal and financial consequences of coding errors create compelling arguments against complete automation without human oversight.
For example, in 2025, the U.S. Department of Justice secured a $23 million settlement over an automated coding system that upcoded emergency department visits, demonstrating real legal consequences when AI coding operates without sufficient oversight.
2. Complexity and Contextual Understanding Limitations
The complexity of the ICD-10-CM system, with nearly 68,000 diagnostic codes, combined with frequent updates and changes to coding standards, increases the risk of errors and inconsistencies.
Plus, some complex cases require sharp analytical thinking and problem-solving skills that AI currently lacks. Human coders excel at handling ambiguous cases, providing contextual insight that AI misses, and ensuring codes accurately reflect the patient's condition and treatment.
CombineHealth’s Amy (AI Medical Coding Agent) routes about 15% of charts with ambiguous information or high complexity for human review.
3. Ethical Concerns and Bias Mitigation
AI medical coding is powerful, but it comes with real ethical responsibilities. When you give an algorithm the authority to translate clinical care into billable codes, you also give it the power to shape patient records, influence reimbursement, and affect long-term health outcomes.
In medical coding, that means coders, clinicians, and auditors lose visibility into why a code was assigned or how a decision was made.
In fact, recent research shows that some frontier AI models, when strongly pushed toward a goal, have attempted to bypass or disable safety measures.
Will Autonomous Coding Replace Medical Coders?
No — it shifts coders from production coding of routine charts to exception handling, audits, and complex cases. Low-complexity throughput needs fewer people; judgment work becomes more valuable, which also eases coder-shortage pressure rather than adding layoffs.
Amy routes the ~20% of charts that are low-confidence or flagged by client-configured thresholds to coders, who focus on the cases that genuinely need expertise — and senior auditors on the lowest-confidence ones.
How Should You Evaluate an Autonomous Medical Coding Vendor?
To evaluate an autonomous medical coding vendor, look past headline accuracy. Ask how accuracy is measured (claim-line vs. claim-level), the automation rate, denial reduction, payer-awareness, explainability and audit trail, documentation/CDI capture, and implementation time.
Here are some KPIs to track in pilot:
Amy gives an explainable rationale and audit trail for every code, exposes client-specific rules as configurable settings, and reports the claim-line and outcome metrics above — the evidence a CFO needs to justify the investment.
Ready to Augment Your RCM Team With Autonomous Medical Coding?
As the debate around full autonomy versus human oversight continues, one thing is increasingly clear: the future of medical coding isn’t about choosing between humans or AI—it’s about designing systems where both do what they do best.
Fully autonomous coding, without safeguards, raises legitimate concerns about bias, transparency, and accountability. But autonomy paired with responsible human review creates something far more powerful than either could achieve alone.
This is exactly the vision behind CombineHealth’s autonomous medical coding solution. Amy, our AI medical coding agent, complements the work of medical coders by:
- Coding high-confidence encounters end-to-end
- Flagging ambiguous or risky cases for human review
- Explaining every decision she makes
- Continuously learning from feedback, guidelines, and payer rules
Book a demo to see Amy in action!
FAQs
How accurate is autonomous medical coding compared to human coders?
Modern autonomous coding systems consistently achieve accuracy levels equal to or higher than human coders, especially on routine, high-volume encounters. Many exceed 95–99% accuracy when trained on high-quality data. However, accuracy varies by specialty and documentation quality, which is why human oversight remains essential for complex cases.
How do confidence thresholds and human review workflows work in autonomous coding?
Each chart receives a confidence score based on how certain the AI is about its code selections. High-confidence encounters are auto-coded, while low-confidence, ambiguous, or high-risk cases automatically route to human coders. This ensures efficiency without sacrificing safety, with humans reviewing only the cases that genuinely need expert judgment.
What are the common compliance and audit risks with autonomous coding?
Major risks include upcoding, insufficient documentation support, missing modifiers, ignoring payer-specific rules, and a lack of transparent reasoning. If left unchecked, these issues can trigger denials, repayments, or even legal exposure. Responsible systems mitigate this through built-in compliance checks, explainability, confidence thresholds, and continuous human oversight.
How do regulatory bodies (e.g., CMS, DOJ, OIG) view autonomous coding, and what are the latest compliance guidelines?
CMS, DOJ, and OIG do not prohibit autonomous coding but expect strong human oversight, audit trails, transparency, and clear documentation support. The DOJ has already penalized up-coding tied to automated systems.
What types of claims are most vulnerable to risk if coded autonomously without human oversight?
High-complexity encounters pose the most risk: emergency medicine, surgical cases, critical care, multi-system conditions, rare diagnoses, and charts with unclear or incomplete documentation. These cases require nuanced clinical judgment and are more likely to be audited. Without human review, they may be mis-coded or flagged for compliance violations.
We can't hire enough coders. Is autonomous coding mature enough now?
Yes — in 2026 it runs in production, autonomously coding a majority of routine charts and routing complex ones to your remaining coders. It's most valuable exactly when hiring is hard, because throughput no longer depends on headcount.
Our AI coding pilot hit high accuracy but denials didn't improve. Why?
Accuracy alone doesn't prevent denials. If the system isn't payer-aware — applying LCDs/NCDs and learning from denial patterns — technically correct codes still get downcoded or denied for medical necessity. Evaluate payer-outcome learning, not just code-match accuracy.
We already use CAC but productivity hasn't improved. What's missing?
CAC only suggests codes; a human still validates every chart, so it rarely removes work. Autonomous coding completes high-confidence charts end-to-end and escalates only exceptions — that's where the productivity actually comes from.
We want to automate coding but still pass payer audits. Is that realistic?
Yes, if the system is explainable and produces an audit trail — showing which documentation and rules justify each code. Keep human review on high-risk charts, and the automated work is defensible in an audit.
We're seeing more payer denials despite accurate coding. Can autonomous coding help?
Often the issue is documentation or payer rules, not the codes. Payer-aware autonomous coding flags documentation that won't survive review and applies payer-specific requirements before submission, reducing denials on otherwise-correct claims.
Leadership wants ROI before approving. What metrics matter most?
Coding-related denial rate, captured revenue (including recovered undercoding), automation rate, and cost-to-code — measured in a time-boxed pilot. Productivity alone understates the value; the reimbursement metrics make the board case.