New Patient CPT Code: The Complete Guide
This guide explains new patient CPT code selection, the three-year rule, visit levels, modifiers, consults, preventive visits, and common billing mistakes that lead to denials.
June 1, 2026


Key Takeaways
• New patient codes (99202–99205) apply when no same-specialty provider in the group saw the patient in three years.
• The visit level is set by medical decision-making (MDM) or total time—document which one you used.
• Consults (99242–99245), preventive physicals (99381–99387), and the G2211 add-on each follow their own rules.
• The new-vs-established call drives errors: billing "new" for an established patient triggers recoupment.
• AI coding tools cut errors by automating code selection, unit validation, and documentation checks before submission.
New patient visits are everyday work for most coders—and one of the easiest places to lose money when the coding is wrong.
In fact, new patient CPT codes (99202–99205) accounted for $256.1 million in improper Medicare payments, according to CMS.
Most of that risk comes down to two factors that determine how a new patient visit is coded:
- Patient status: whether the patient is truly new or established.
- Visit level: which level (99202–99205) the documentation supports, based on MDM or total time.
If you get them wrong, the claim is either downcoded and recouped or undercoded and underpaid.
This guide walks through the new patient CPT code families, how to pick the right level, the modifiers and pairings that matter, and the mistakes that trigger the most denials.
What Are New Patient CPT Codes?
New patient CPT codes are a subset of Evaluation and Management (E/M) codes used to report an office or outpatient visit with a patient who is new to the provider.
They apply when a patient hasn't received a professional service from that physician—or another physician of the same specialty and subspecialty in the same group practice—within the past three years.
New patient CPT code set includes four codes (99202 through 99205), each representing a higher level of visit complexity, from straightforward to high. Which one you report depends on the medical decision-making (MDM) involved or the total time spent on the visit.
Like the rest of the CPT code set, new patient CPT codes are maintained by the American Medical Association (AMA).
New Patient vs. Established Patient: The Three-Year Rule
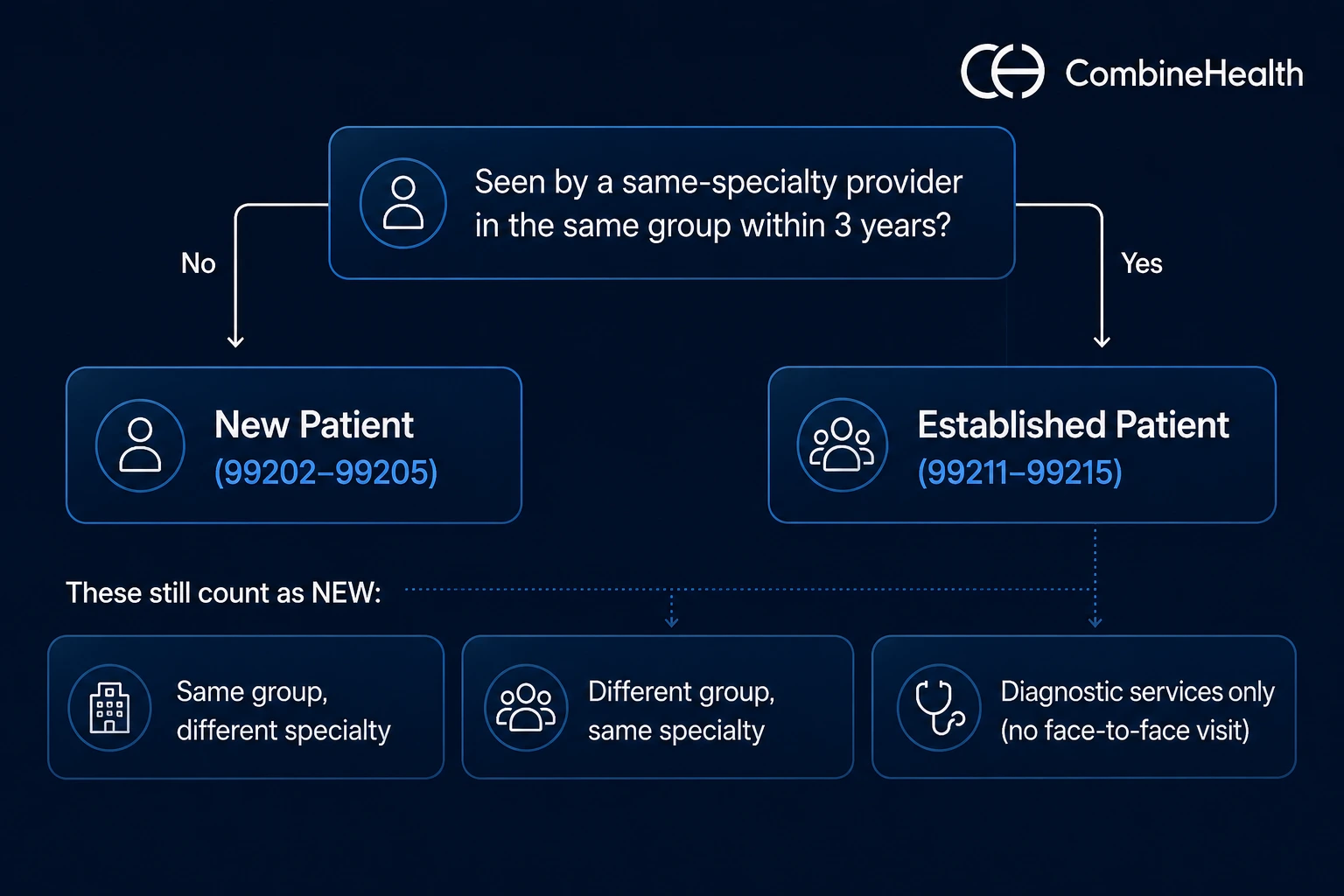
The three-year rule of determining whether a patient should be considered ‘new’ or ‘established’ is straightforward: a patient is new unless a same-specialty provider in the same group has seen them within the past three years.
Getting it wrong is the most common new patient coding error, and it costs both ways: billing "new" for an established patient triggers recoupment, while billing "established" for a new patient underpays the visit.
But three scenarios trip coders up most often, and in each one the patient still counts as new:
- Same group, different specialty: a patient seen by a cardiologist is still new to the internal medicine provider in that same group.
- Different group, same specialty: a patient transferring from a competing practice is always new, no matter how recently they were seen elsewhere.
- Diagnostic services only: a patient whose imaging your group's radiologist read, but who never had a face-to-face visit, is still new.
The distinction is worth the care: new patient codes pay more, so billing "new" when the patient is established triggers recoupment, while the reverse underbills the visit.
Types of New Patient CPT Codes
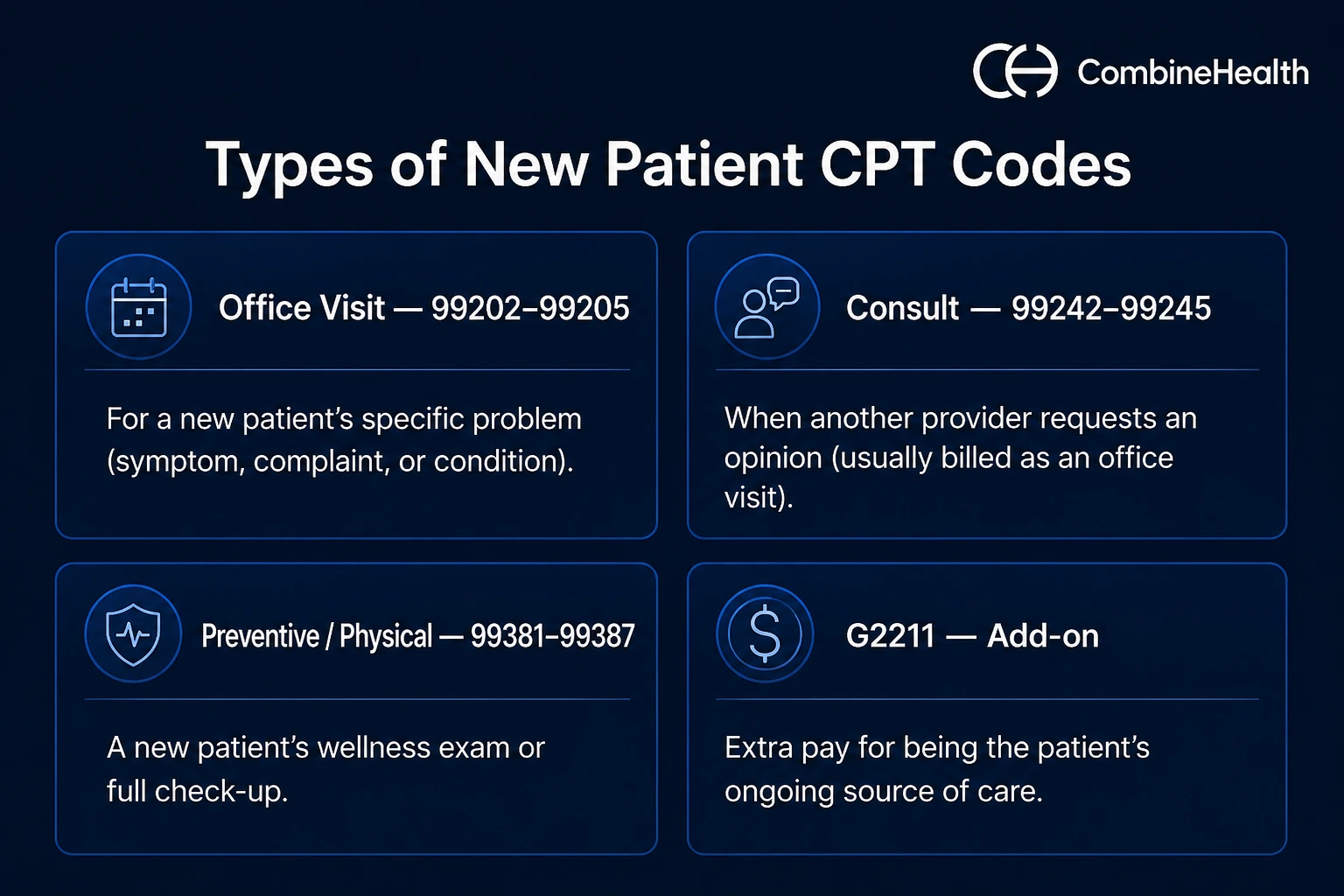
1. New Patient Office Visit CPT Codes (99202–99205)
New patient office visit codes (99202–99205) are used when a provider treats a new patient for a specific problem—a symptom, complaint, or condition.
You choose one of the four levels based on the complexity of the medical decision-making (MDM), or the total time spent on the day of the visit (which includes work such as chart review and documentation, not just face-to-face time).
Note: 99201 was the old level-one code, but it was deleted in 2021. The range now starts at 99202.
2. New Patient Consult CPT Codes (99242–99245)
Consult codes (99242–99245) are used when another provider asks your physician to evaluate a new patient and give an opinion on a specific problem.
You pick the level by MDM or by meeting a minimum time.
There's a catch, though: CMS stopped paying for consultation codes in 2010, and most commercial payers followed, so a new patient "consult" is usually billed as a regular office visit (99202–99205) instead.
Note: 99241, the old lowest consult level, was deleted in 2023.
3. New Patient Physical (Preventive) CPT Codes (99381–99387)
Preventive codes (99381–99387) are used for a new patient's wellness exam or physical, a full check-up, rather than a visit for a specific problem.
You choose the code by the patient's age, not by MDM or time. If the provider also handles a separate problem during the same visit, you can add an office visit code (99202–99205) with modifier 25.
4. G2211: The Longitudinal Care Add-On
G2211 is an add-on code that pays a provider extra for being a patient's ongoing source of care, billed on top of a regular office visit.
For example, a primary care physician manages a patient’s long-term health. Medicare started paying it separately in 2024; before then, the code wasn't reimbursed at all.
G2211 applies only when the provider plans to take on the patient's ongoing care. A one-time or acute-only visit with no continuing relationship doesn't qualify.
Note: Coverage for G2211 outside traditional Medicare varies. Some commercial and Medicare Advantage plans cover it, others don't, so always check payer policy.
Recommended reading: ER CPT Codes: The Complete Guide
New Patient ICD-10 Codes and Billing Modifiers
ICD-10 codes are the diagnosis codes that tell a payer why a service was provided. On a new patient claim, each ICD-10 code must support the CPT code it's billed with—otherwise the claim is denied or downcoded for lack of medical necessity.
Key New Patient Billing Modifiers
These are some of the common new patient billing modifiers that come up most on new patient visits.
Common Challenges in New Patient CPT Coding and Billing
Most new patient errors trace back to a handful of recurring pitfalls.
Watch for these:
- Patient-status misclassification: A failed three-year, same-specialty, same-group look-back is the single most common new-vs-established error.
- MDM-versus-time confusion: Selecting a level without documenting which method justified it, leaving 99204 and 99205 exposed on audit.
- Consult miscoding: Billing 99242–99245 to payers who don't recognize them, then absorbing the denial instead of reporting 99202–99205.
- G2211 misuse: Appending it to preventive or wellness visits, or to one-off new patient encounters with no longitudinal intent.
- Missing modifier 25: Bundling a separately identifiable problem visit into a same-day preventive exam and forfeiting the second line.
Get New Patient CPT Coding Right, Every Time, with AI
Every pitfall in this guide—the new-vs-established call, the MDM-versus-time decision, a missed modifier 25—comes down to applying the right rule correctly, claim after claim, under time pressure.
Doing this manually at scale makes errors almost inevitable. Even skilled billing teams struggle to avoid them.
That's the kind of repetitive, rules-heavy work automation handles well.
CombineHealth's Amy (AI coding solution) is built for it:
- Automated code selection: picks the correct new patient code straight from the documentation.
- Unit validation: confirms units are right before the claim is submitted.
- CDI checks: surface documentation gaps while there's still time to fix them.
Once deployed, you can expect fewer visits to come back downcoded or denied, and far less rework for a team coding new patient visits all day.
Book a demo to see how CombineHealth supports your coding team's accuracy on new patient visits!
FAQs
1. What is the CPT code for a new patient office visit?
New patient office visits are reported with CPT codes 99202–99205. The level is chosen by medical decision-making or total time on the date of the encounter.
2. Is there still a CPT code 99201?
No. The AMA deleted 99201 on January 1, 2021, when the office and outpatient E/M guidelines were revised. The new patient range now starts at 99202.
3. What is the CPT code for a new patient consult?
Office consult codes 99242–99245 still exist in CPT, but CMS and most commercial payers no longer reimburse them. In most cases, you'll report a standard new patient office visit (99202–99205) instead.
4. What is the CPT code for a new patient physical?
A new patient's physical is reported with a preventive medicine code, 99381–99387, selected by the patient's age rather than by time or MDM.
5. Can G2211 be billed with a new patient visit?
Yes. G2211 can be reported with 99202–99205 when the provider intends to establish an ongoing, longitudinal care relationship. A one-time visit with no continuing relationship doesn't qualify.






