8 Stages of RCM Cycle in Medical Billing: The Complete Process Explained
Learn the 8 stages of the healthcare revenue cycle, common revenue leaks, and how to reduce denials, improve collections, and optimize RCM performance.
April 3, 2026


Key Takeaways:
• The RCM cycle spans eight interconnected stages—from patient registration to final payment—and breakdowns in any stage directly impact revenue outcomes.
• A majority of denials originate from preventable upstream errors like incorrect registration data, missing prior authorizations, and incomplete documentation.
• Clinical documentation and coding form the foundation of accurate reimbursement, but gaps in specificity or alignment often result in undercoding, compliance risks, or claim rejections. Strong coordination between CDI and coding is critical to prevent downstream issues.
• Clean claim submission and accurate payment posting depend on payer-specific validation and proper reconciliation, not just data entry. Without this, underpayments and missed discrepancies quietly erode revenue.
• High-performing organizations treat RCM as a connected system, focusing on root-cause resolution rather than reactive denial management.
Your billing team submitted the claim. The work was done, the patient was seen, and the documentation was filed. But a denial came back anyway.
It happens to most health systems, and the reason usually traces back to something that went wrong long before the claim was submitted.
And the worst part is the denial queue grows faster than the team can work it, so recoverable revenue gets written off by default. According to HFMA, 65% of denied claims are never reworked or resubmitted.
What's driving this gap is the distance between eight stages that are supposed to function as one process — from the moment a patient books an appointment to the moment their balance is paid. When those stages don't share information, revenue slips through every handoff. This means a documentation gap at stage four shows up as a denial at stage eight. And by the time anyone notices, the deadline to appeal is two weeks out.
This article walks through all eight stages of the RCM cycle in medical billing: what each one does, where money typically gets lost, and what it takes to run them without leaving revenue on the table.
What is RCM Cycle in Medical Billing?
The Revenue Cycle Management (RCM) cycle in medical billing is the end-to-end process healthcare organizations use to track, manage, and collect revenue for the services they provide.
It starts the moment a patient schedules an appointment and continues until the final payment (from either the payer or the patient) is collected and reconciled.
8 Stages of the RCM Cycle in Medical Billing
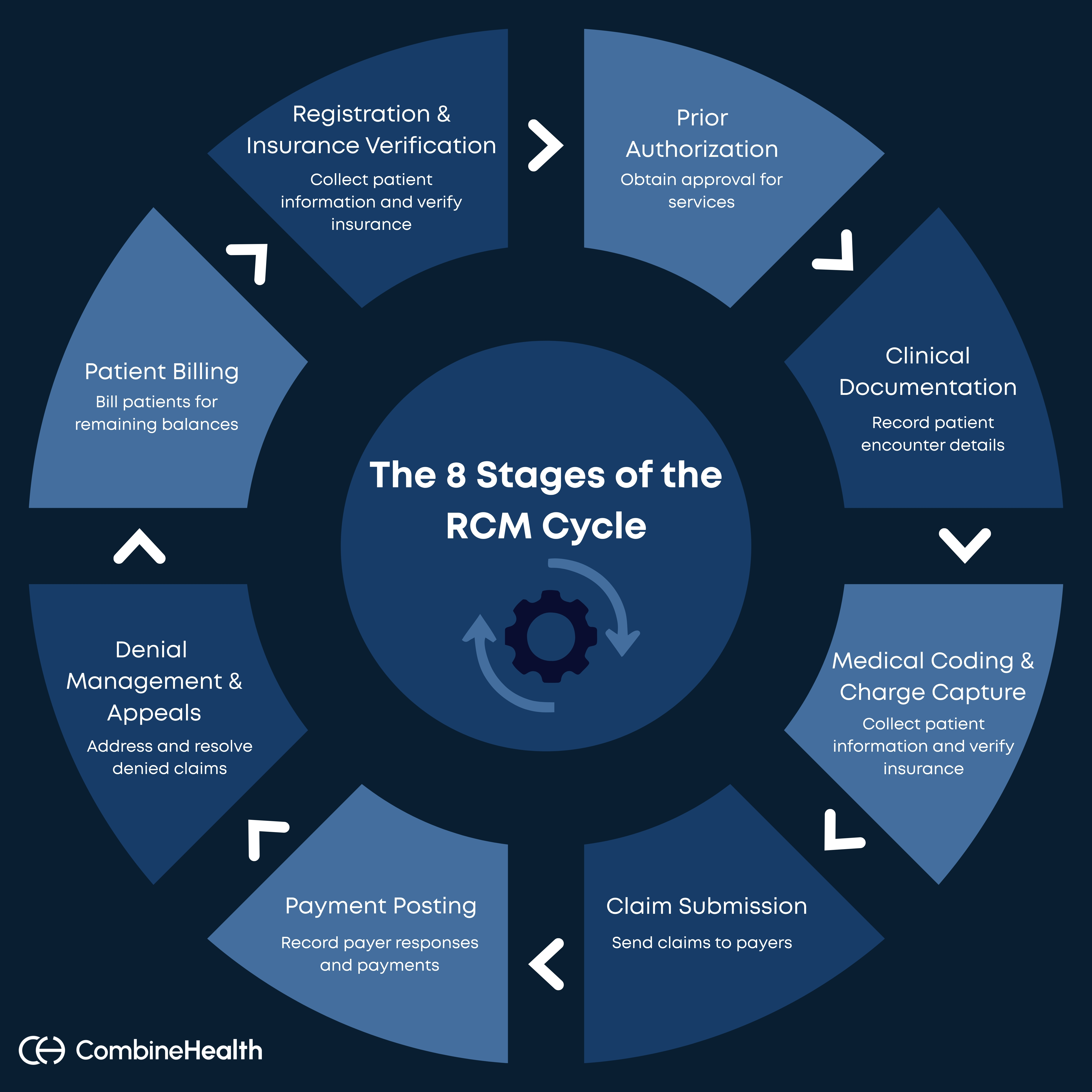
In the sections below, we’ll walk through each stage of the RCM cycle — what happens, what needs to go right, and where organizations typically run into challenges:
1. Registration & Insurance Verification
Registration is where the patient’s demographic information, insurance details, and appointment data are collected before the patient arrives.
Most billing teams treat this as an administrative handoff. The better ones treat it as the first line of denial prevention.
That’s because registration and eligibility errors have been the leading cause of claim denials every year since 2016, now accounting for nearly 27% of all denials, according to HFMA.
The errors driving that number tend to follow these familiar patterns:
- Insurance information collected over the phone and never verified against the payer
- Demographic fields entered incorrectly
- Appointment types that don't align with what the payer covers
- Coverage that lapsed between booking and the visit date
If you think about it, none of these are complicated problems. They're data problems, and data problems at stage one show up as denied claims at stage six.
What This Stage Needs to Get Right
- Collect complete insurance and demographic information at the time of booking. This includes full legal name, date of birth, insurance ID, group number, and primary payer.
- Run a verification window 24 to 48 hours before the appointment, not at check-in when there's no time to fix anything.
- Flag appointment types that typically require prior authorization so the process can start before the visit.
- Confirm coverage is active, not just on file.
2. Prior Authorization
Prior authorization sits at the intersection of clinical care and billing operations, and it creates problems for both.
Before certain procedures, medications, or services are approved for coverage, payers require providers to obtain sign-off in advance.
According to the AMA's prior authorization survey, physicians complete about 40 prior authorizations per week, with most of those requests often or always getting denied. The revenue impact compounds in two scenarios:
- When PA delays push procedures past authorization windows, when authorizations expire before the service date
- When the PA was never initiated at the scheduling stage, and only surfaces as a problem at claim submission
What Should Be Fixed
- Build a PA check into the scheduling workflow, not the billing workflow. When an appointment is booked, the system should flag whether that service, for that payer, requires authorization and trigger the request immediately.
- Track authorization expiration dates actively; an auth obtained three weeks before a procedure can lapse if the appointment shifts.
- Document every PA request, approval, and denial with timestamps, because payer audits and appeals both depend on that paper trail.
3. Clinical Documentation of Patient Encounter
Clinical documentation is the record of what occurred during the patient encounter: the presenting complaint, the clinical findings, the assessment, the treatment plan, and the procedures performed.
It’s also the foundation on which every subsequent stage of the revenue cycle is built:
- Coding pulls from it
- Claims reference it
- Appeals depend on it
When the documentation is incomplete or inconsistent, the revenue impact compounds across every stage downstream. In fact, CMS's data found that 82% of Medicaid improper payments resulted from insufficient documentation.
How to Fix Documentation Errors
Physicians and clinical staff need documentation that captures not just what was done, but why it was clinically necessary. And the specificity of the language matters: "patient presented with chest pain" supports a different level of service than a detailed account of history, exam findings, and medical decision-making.
Plus, real-time documentation using medical scribes is a good way to produce complete and accurate records. But even well-documented encounters can have gaps that only surface when a coder reviews the chart. A physician might document a procedure clearly but leave the clinical indicators for a secondary diagnosis unstated.
This is where clinical documentation improvement helps. CDI specialists review charts before coding to identify documentation gaps, such as:
- Missing specificity
- Unlinked diagnoses
- Procedures documented without supporting medical necessity language
- Conditions that were treated but never formally documented
So, when CDI and coding work from the same chart at the same time, those gaps get resolved with a provider query before the claim is built.
4. Medical Coding and Charge Capture
Medical coding is where the clinical record becomes a billable claim. Every diagnosis, procedure, and service gets translated into a standardized code: ICD-10 for diagnoses, CPT for procedures, HCPCS for supplies and services. And those codes determine exactly what the payer will consider reimbursing and how much.
The stakes of getting this right are high in all directions.
- Undercoding leaves revenue uncaptured
- Overcoding creates compliance exposure
- Coding errors of any kind have a direct line to denials
The most common coding failures at this stage are familiar to any billing team that reviews denials regularly:
- Diagnosis codes that don't support the level of service billed
- Procedures coded without the modifiers payers require
- Unbundling errors
- E/M levels that don't match the documented complexity of the visit
Charge capture is the parallel problem. A procedure performed but never coded is revenue that simply disappears.
What This Stage Needs to Get Right
Coding accuracy depends on documentation quality, which is why the CDI work from stage three directly determines what's possible here.
For challenging environments like the Emergency Department, autonomous coding tools are increasingly being used to handle high-confidence, high-volume encounters — standard procedure codes, straightforward E/M visits, repeat claim types with predictable payer rules.
Recommended Reading: Autonomous Medical Coding in Healthcare RCM
5. Claim Submission
A claim submission is the point where all the work from the previous four stages either pays off or doesn't. The coding is done, the documentation is referenced, and the charge is captured. Now the claim goes to the payer, and how it's built determines whether it comes back paid, rejected, or denied.
The metric that governs this stage is the clean claim rate: the percentage of claims that pass all payer edits on first submission without manual intervention.
The errors that derail clean claim submission are almost always preventable. This includes:
- Missing or incorrect patient identifiers
- Invalid diagnosis-to-procedure code combinations
- Modifier errors
- Missing prior authorization references
- Timely filing deadline misses
How to Submit Clean Claims
Every claim should pass through a scrubbing layer before it reaches the clearinghouse. That scrubbing should be payer-specific, updated regularly, and configured to flag high-risk claim types rather than treating all claims the same.
6. Payment Posting
Once a payer processes a claim, they send back a payment response to the provider. This response typically comes in the form of an Electronic Remittance Advice (ERA) or, in some cases, a paper Explanation of Benefits (EOB).
Payment posting is the process of recording that response into your billing system.
The process involves three key actions:
- Receiving the payer’s response: After claim adjudication, the payer communicates the amount paid, the amount denied, reason codes, and adjustments through an ERA.
- Posting payments and adjustments: The billing team then applies the payment amount to the correct claim and service lines, records adjustments based on payer contracts, and marks the claim as denied, partially paid, or paid.
- Reconciling payments: This is where payment posting becomes more than just data entry. Billing teams compare what was expected vs. what was received and flag discrepancies, such as underpayments, unexpected adjustments, or missing payments.
What This Stage Needs to Get Right
Payment posting depends on how accurately payer responses are interpreted and applied — because this is where revenue is finalized, not just received.
Billing teams (or systems) need to know:
- What the allowed amount should be
- How payer-specific adjustments should be applied
- When a payment is correct vs. silently underpaid
Without that context, posting becomes blind data entry instead of financial validation.
7. Denial Management and Appeals
Denial management is the process of identifying, analyzing, and resolving denied claims to recover revenue. And appeals is when providers formally challenge a payer’s denial by submitting corrected claims, supporting documentation, or clinical justification to overturn the decision and secure reimbursement.
At a high level, this stage involves three core activities:
- Identifying and categorizing denials: Every denied claim comes with a denial reason code, payer explanations, and some indication of what went wrong. At this stage, the goal is to make sense of that information by grouping denials into categories such as eligibility issues, missing prior authorizations, coding errors, lack of medical necessity, or documentation gaps.
- Investigating the root cause: Once denials are categorized, the next step is to investigate where the breakdown actually occurred. This often means tracing the issue back to earlier stages in the revenue cycle — whether it originated during registration, prior authorization, documentation, coding, or billing. In some cases, the issue may even be on the payer’s side.
- Correcting and appealing the claim: After identifying the root cause, teams take action to resolve the denial. This may involve correcting errors such as missing modifiers or inaccurate patient information, attaching supporting documentation, and resubmitting the claim. In cases where the payer disputes the claim, teams move into the appeals process, which requires drafting detailed appeal letters backed by clinical justification and coding rationale.
How Denials Can Be Prevented
Denial management only works when it moves beyond rework and into root-cause correction.
If teams focus only on reworking denials and submitting appeals, they remain stuck in a reactive cycle. The real leverage comes from identifying patterns — recurring denial reasons, payer-specific issues, and consistent breakdowns in upstream processes like documentation, coding, or authorization.
This is where automation is starting to make a difference.
.webp)
8. Patient Billing
Patient billing is the final stage of the revenue cycle, where any remaining balance after payer reimbursement is billed directly to the patient. The remaining balance may include costs like:
- Deductibles
- Co-pays
- Co-insurance
- Non-covered services
The process typically involves generating patient statements, sending them through mail or digital channels, and providing payment options such as online portals or payment plans.
However, this stage introduces a very different dynamic into the revenue cycle.
In many cases, patients:
- May not fully understand their bills
- May delay or avoid payments
- May require multiple follow-ups or support
What This Stage Needs to Get Right
Patient billing works best when it reduces friction for the patient while maintaining clarity and accuracy.
That means:
- Bills must be easy to understand
- Payment options must be simple and accessible
- Communication must be timely and consistent
If patients don’t understand what they owe or why, delays are almost guaranteed. And if the payment experience is complicated, even willing patients may drop off.
Stop Treating RCM as a Set of Isolated Tasks!
While the RCM cycle is often presented as a sequence of steps, in practice, it functions more like a connected system.
What happens in one stage directly affects the next:
- Errors during registration lead to eligibility denials
- Poor documentation limits coding accuracy
- Coding mistakes result in claim rejections
- Missed discrepancies during payment posting impact A/R follow-up
This is why high-performing organizations don’t treat RCM as isolated tasks. They focus on how information flows across the entire cycle and where breakdowns occur.
This is exactly where an AI-driven RCM solution like CombineHealth brings value — connecting each stage, identifying breakdowns in real time, and ensuring revenue doesn’t slip through the cracks.
Book a demo to see how CombineHealth helps you run a truly connected revenue cycle.
FAQs
What is revenue cycle management in healthcare?
Revenue cycle management (RCM) is the process of tracking and collecting revenue from patient care, from appointment scheduling to final payment. It includes registration, coding, billing, claims submission, payment posting, and denial management.
Can you recommend the best software for healthcare revenue cycle management?
The best RCM software depends on your needs. Options range from end-to-end AI platforms like CombineHealth to EHR solutions like Epic and AthenaHealth. Look for accuracy, automation, integration with EHRs, and strong denial prevention capabilities.
What tools or dashboards are recommended for monitoring healthcare revenue KPIs?
Use dashboards that track real-time KPIs like A/R days, denial rates, and net collection rate. Tools like Tableau, Power BI, and built-in RCM analytics platforms (or AI-driven tools like CombineHealth’s analytics layer) help identify bottlenecks and performance gaps quickly.
How can I improve revenue cycle metrics for better financial performance?
Focus on upstream accuracy—clean registration, verified eligibility, complete documentation, and precise coding. Implement claim scrubbing, track denial patterns, and fix root causes. Automation and real-time analytics can significantly reduce errors and improve collections.
How do revenue cycle metrics impact overall healthcare practice efficiency?
RCM metrics directly reflect operational efficiency. Poor metrics—like high denial rates or long A/R days—indicate process breakdowns, staff inefficiencies, and cash flow delays. Strong metrics mean smoother workflows, faster reimbursements, and less administrative burden.
What are the most important KPIs to track in healthcare revenue cycle management?
Key KPIs include net collection rate, days in A/R, denial rate, first-pass claim acceptance rate, and cost to collect. These metrics reveal how efficiently revenue is captured, processed, and collected across the entire cycle.
How is the healthcare revenue cycle management market expected to evolve in the next few years?
RCM is shifting toward AI-driven automation, real-time decision-making, and end-to-end workflow integration. Expect increased adoption of autonomous coding, predictive denial prevention, and unified platforms that replace fragmented point solutions.
What are the main challenges faced in healthcare revenue cycle management?
Common challenges include rising denial rates, staffing shortages, complex payer rules, fragmented systems, and documentation gaps. These issues create inefficiencies, increase manual workload, and delay payments, ultimately impacting revenue and operational stability.






