Top 15 Claim Denials in Healthcare RCM
Discover the 15 most common healthcare claim denials, why they occur, how to resolve them, and proven strategies to prevent revenue loss and improve reimbursement.
June 5, 2026

Key Takeaways
• CO-16, CO-197, CO-50, CO-29, and CO-45 are among the most common denial codes, but most denials fall into a few core categories: eligibility, authorization, coding, documentation, and billing errors.
• Many denials can be resolved without an appeal by identifying the root cause, correcting the claim, and resubmitting it with the required information or documentation.
• CARCs and RARCs should always be reviewed together to understand exactly why a claim was denied and determine the appropriate next step.
• Most claim denials are preventable through proactive eligibility verification, prior authorization management, claim scrubbing, and staff training on payer-specific requirements.
• A structured denial management process helps reduce revenue leakage, improve reimbursement rates, and identify recurring denial patterns before they become systemic problems.
Claim denials are becoming an increasingly costly challenge for healthcare providers. Recent industry data shows that denial rates are rising across the healthcare sector, with nearly half of providers reporting an increase in denied claims.
In this guide, we'll break down the 15 most common medical billing denial codes, explain what each denial means, why it happens, how to fix it, and the steps providers can take to prevent it from recurring.
15 Most Common Denial Codes (and Fixes)
1. CO-16: Missing Information
CO-16 means the claim is missing required information or contains invalid information that prevents the payer from processing it. The fastest fix is to identify the exact missing or invalid field using the attached RARC, correct the claim, and resubmit it.
Common Causes of CO-16 Denials
How to Fix It
- Pull the RARC(s) attached to the denial before doing anything else
- Identify the exact field flagged
- Correct and resubmit; do not file an appeal if the error is a data entry issue
- Add the missing field type to your pre-submission scrub rules to prevent recurrence
2. CO-197: Prior authorization Missing
CO-197 is a denial code indicating that a required authorization was missing, invalid, expired, or not properly linked to the claim.
Common Causes of CO-197 Denials
How to Fix CO-197 Denials
- Verify whether an authorization exists.
- Review authorization details:
- Authorization number
- CPT/HCPCS codes
- Units approved
- Date range
- Site of service
- If authorization exists:
- Correct the claim.
- Add the authorization number.
- Resubmit.
- If no authorization exists:
- Review payer retrospective authorization policy.
- Submit appeal only when retrospective review is permitted.
- Include strong medical necessity documentation.
How to Prevent CO-197 Denials
- Maintain a payer-specific prior auth rules library — coverage requirements change, and what didn't require auth last quarter may require it now
- Verify at the time of scheduling which CPT/HCPCS codes require authorization for that specific payer and plan
- Capture the authorization number and UTN in structured fields at the time it's obtained — not as a note, not in a free-text box
- Confirm the auth covers the correct site of service, procedure codes, approved units, and date range before the appointment
3. CO-26: Expenses Incurred Prior to Coverage
CO-26 is a denial code indicating that services were rendered before active coverage began under the patient's health plan.
Common Causes of CO-26 Denials
How to Fix CO-26 Denials
- Verify effective and termination dates directly with the payer.
- Determine whether another active plan existed on the date of service.
- Rebill the correct payer if applicable.
- If no coverage existed, follow patient responsibility procedures and applicable regulations.
How to Prevent CO-26 Denials
- Verify eligibility at every visit — not just new patients, not just annually
- Confirm the effective date specifically, not just that a policy is active; active status alone doesn't tell you when coverage started
- Re-verify whenever a patient reports a coverage change, even mid-treatment
- Flag patients presenting with new insurance cards or unfamiliar plan IDs for real-time eligibility checks before service is rendered
4. CO-50: Medical Necessity Not Met
CO-50 is a medical necessity denial based on LCDs, NCDs, or commercial payer medical policies.
Common Causes of CO-50 Denials
How to Fix It
- Pull the specific LCD, NCD, or commercial coverage policy before writing a single word of the appeal — map your clinical documentation against the payer's criteria, not against general medical reasoning
- Build your appeal packet around the physician's notes showing clinical rationale, documentation of prior conservative treatment, diagnostic results supporting the indication, and a direct citation to the policy language you're responding to
- For Medicare claims where coverage is uncertain before service is rendered, issue an ABN — it protects the practice and makes the patient's financial responsibility clear upfront if the claim is denied
- If the same procedure is coming back CO-50 from the same payer repeatedly, the fix isn't in the appeal queue — trace it back to the diagnosis coding or clinical documentation feeding the claim
5. N115: Insufficient or Missing Documentation
N115 indicates the payer needs additional documentation or specific coverage requirements were not met.
Common Causes of N115 Denials
How to Fix It
- Identify the specific LCD referenced in the denial — CMS publishes all active LCDs at cms.gov; look up the exact determination that applies to the billed service
- Compare your documentation and coding against the LCD's criteria line by line — note precisely what's missing or misaligned
- Gather the missing documentation, update coding or modifiers where appropriate, and submit an appeal that cites the specific LCD sections your evidence now satisfies
- Before billing high-risk services, run the LCD check upstream — confirm covered diagnoses, required documentation elements, and modifier rules before the claim is submitted
6. CO‑11: Diagnosis/procedure mismatch
CO-11 occurs when the diagnosis code on the claim doesn't clinically support the service billed under the payer's rules.
Common Causes of CO-11 Denials
How to Fix It
- Go back to the medical record and confirm the correct primary diagnosis and that it supports the CPT billed
- If the diagnosis was miscoded, correct it and resubmit as a corrected claim — this is a billing correction, not an appeal
- If the coding is accurate and the documentation supports necessity, appeal with the chart notes showing the clinical relationship between the diagnosis and the procedure
- Build front-end edits that flag diagnosis-procedure combinations known to trigger CO-11 before claims leave the system
7. CO‑4: Modifier errors
CO-4 denial code means the modifier used doesn't fit the procedure code, or a required modifier was omitted entirely.
Common Causes of CO-4 Denials
How to Fix It
- Review the NCCI edit and the payer's modifier policy for the specific CPT — confirm whether the modifier used was appropriate for that clinical scenario
- Correct or add the proper modifier with supporting documentation and resubmit as a corrected claim
- If the modifier was correct and the denial is a payer error, appeal with documentation demonstrating why the modifier applies
- Configure PM or clearinghouse edits to flag invalid CPT-modifier combinations at the time of claim building — CO-4 is one of the most preventable denials in the queue
8. CO-29: Timely Filing Limit Exceeded
CO-29 means the claim was submitted after the payer's filing deadline, which typically ranges from 90 to 365 days from the date of service, depending on the plan.
Common Causes of CO-29 Denials
How to Fix It
- If the claim was actually submitted on time, appeal with evidence — clearinghouse confirmation reports, submission logs, or payer acknowledgment records showing timely filing
- If a payer error caused the delay, document it and request an exception with supporting proof
- If the filing window genuinely passed, recovery options are limited — most CO-29 denials without timely filing proof become write-offs
- Prevent recurrence by maintaining a payer-specific filing deadline matrix and building A/R worklist rules that surface near-deadline claims before the window closes
9. CO-256: Service Not Payable Under Managed Care Contract
CO-256 means the billed service is not covered or payable under the provider's managed care contract with that payer.
Common Causes
How to Fix It
- Pull the managed care contract and the payer's benefit policy, and confirm whether the service is contractually payable for this plan and provider type
- If a coding error misclassified the service, correct it and resubmit
- If the service is legitimately excluded under a CO group code, post it as a contractual write-off — you cannot bill the patient for CO adjustments
- Prevent future occurrences by incorporating contract exclusions into scheduling, authorization, and benefit verification workflows before services are rendered
10. PI-252: Additional Documentation Required
PI-252 means the payer won't adjudicate the claim until you send an attachment or additional documentation. This typically includes operative reports, pathology results, chart notes, or an EOB for coordination of benefits.
Common Causes
How to Fix It
- Read the RARC attached to the PI-252 before doing anything else — it tells you precisely what's missing (N710 for missing notes, N714 for a missing report, etc.)
- Collect the requested documentation and submit it via the payer's document upload portal or with a corrected claim, depending on the payer's process
- Track which procedures consistently trigger PI-252 from the same payers and build standard documentation attachment workflows for those services upfront
- For COB claims, confirm that the primary payer's EOB is always attached before submitting to the secondary — PI-252 on secondary claims is almost always a missing EOB
11. CO-32: Patient Not an Eligible Dependent
CO-32 is an eligibility denial indicating that dependent coverage was inactive, terminated, or not properly reflected in the payer's enrollment records.
Common Causes of CO-32 Denials
How to fix it:
- Confirm directly with the payer whether the dependent coverage was active on the date of service and when it terminated
- If the payer's records are incorrect, have the subscriber contact their employer or plan to update enrollment, then request reprocessing with proof of active coverage
- If the dependent is genuinely ineligible, move the balance to self-pay or check for alternate active coverage before writing it off
- At registration, verify dependent eligibility and relationship status — not just that a policy is active, but that this specific patient is recognized as a covered member under it
12. CO-45: Charge Exceeds Payer's Allowable Amount
CO-45 is a contractual adjustment indicating that payment has been reduced to the payer's negotiated reimbursement rate.
Common Causes of CO-45 Adjustments
How to fix it:
- Confirm the allowed amount matches your current contract for that payer, plan type, and procedure code before posting the adjustment
- If the allowed amount is correct, post CO-45 as a contractual write-off — do not bill the patient for the CO portion
- If the allowed amount appears wrong, contact the payer with the relevant contract language and request a reprocessing or rate correction
- Audit CO-45 adjustments periodically against contracted rates — systematic underpayment by a payer doesn't always generate a denial; it shows up quietly in the CO-45 line
13. PI-204: Service Not Covered Under the Benefit Plan
PI-204 tells you the patient's plan simply doesn't include this service. Before accepting that at face value, it's worth confirming the denial reflects an actual exclusion — and not a fixable coding or authorization issue wearing one.
Common Causes of PI-204 Denials
How to fix it:
- Before accepting the denial, check whether a coding error or missing authorization is the real cause — both can produce PI-204 on claims where the service itself is covered
- If the denial is legitimate, verify the group code and applicable regulations before billing the patient for the balance
- Check for secondary coverage before writing off a PI-204 denial — another active plan may cover what this one excludes
- Verify benefits at scheduling, including specific exclusions and network status, so non-covered services are identified and communicated to patients before care is delivered
14. CO-18: Duplicate Claim
CO-18 is a duplicate claim denial triggered when the payer identifies matching claim information for the same patient, provider, date of service, and procedure.
Common Causes of CO-18 Denials
How to fix it:
- Check claim history and the payer portal before taking any action — if the original is paid or in process, stop; resubmitting again adds another duplicate to the queue
- If a correction is needed, use the payer's formal corrected-claim workflow with the appropriate claim frequency code — not a new claim submission
- If the CO-18 is a payer error and the claims are genuinely distinct services, appeal with documentation showing the clinical distinction between the two
- Configure PM system and clearinghouse rules to flag potential duplicate submissions before they go out, and establish a single point of ownership for resubmissions across departments
15. CO-B7: Provider Not Certified or Eligible for This Service
CO-B7 is a provider enrollment denial indicating the payer cannot reimburse the service because of a credentialing or enrollment issue.
Common Causes of CO-B7 Denials
How to fix it:
- Confirm whether the provider was actually enrolled and eligible on the date of service — a taxonomy or NPI error on the claim is a correctable billing issue, not a true enrollment gap
- If the denial is a data error, correct the taxonomy or NPI and request reprocessing
- If the provider genuinely wasn't enrolled, complete enrollment and work with the payer on whether retroactive payment is possible — most payers have limited windows for this
- Maintain a credentialing tracker that surfaces enrollment gaps before new providers see patients — CO-B7 denials are entirely preventable when enrollment is verified at onboarding, not discovered at billing
How to Interpret a Denial (Step-by-Step)
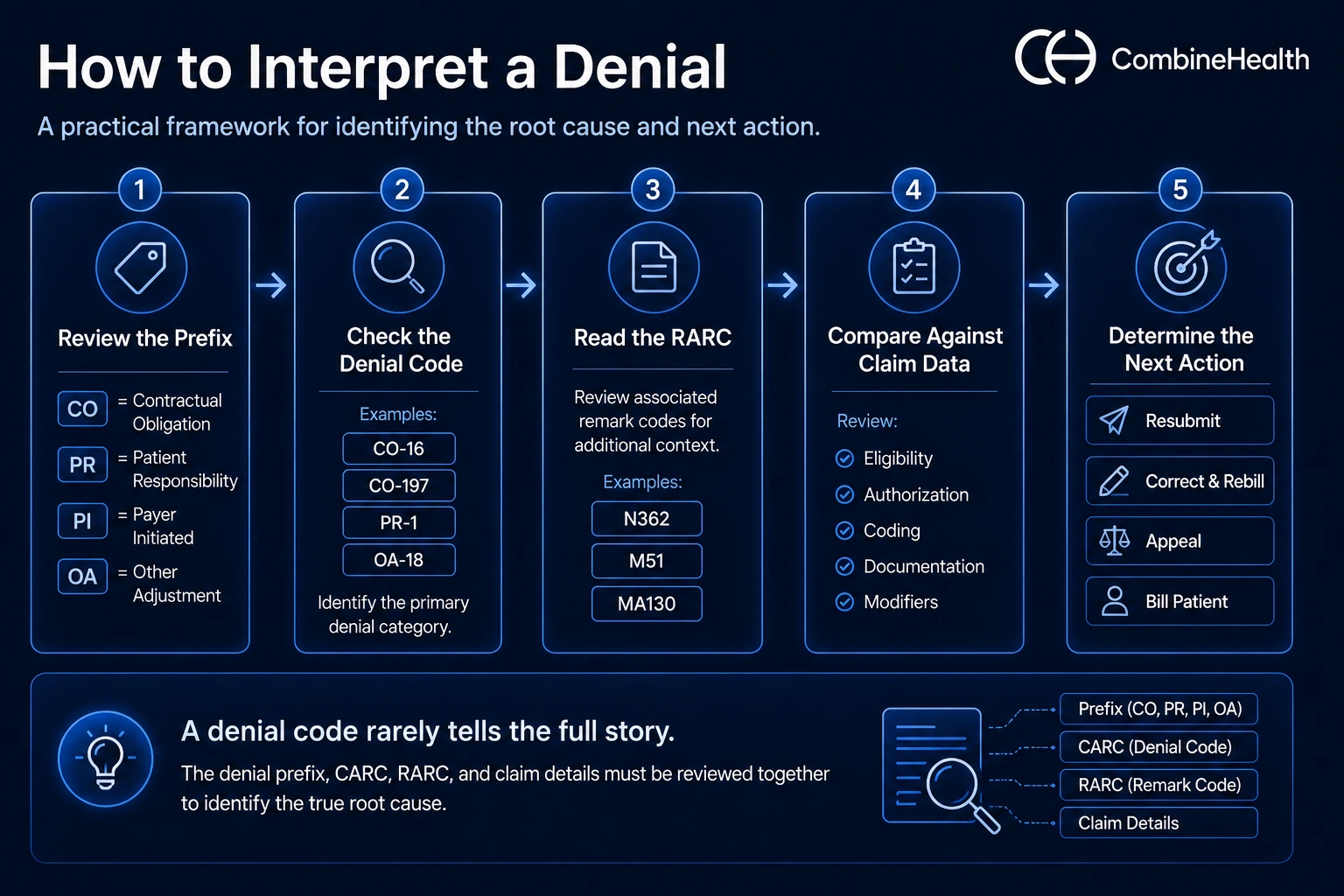
To interpret a denial code, start with the denial code prefix to determine responsibility, then review the denial reason code, associated remark codes, and claim details to identify the root cause and next action.
Here’s how:
- Review the prefix (CO, PR, PI, OA).
- Check the denial code (e.g., CO-16, CO-197).
- Read the RARC for specifics.
- Compare the denial to claim data.
- Determine whether to resubmit, correct, appeal, or bill the patient.
How Do You Address Medical Billing Denials?
The appropriate response depends on the denial reason and whether the issue involves data, documentation, coverage, or patient responsibility.
Resolution Options:
- Correct and Resubmit: Missing or incorrect information.
- Submit a Corrected Claim: Billing or coding errors.
- Appeal: Medical necessity or coverage disputes.
- Bill the Patient: PR denials when permitted.
Denial Prevention Strategies
Most medical billing denials can be prevented by strengthening front-end revenue cycle processes before claims are submitted.
Some best practices to follow:
- Verify insurance eligibility before every visit.
- Obtain required prior authorizations before services are rendered.
- Use claim scrubbing tools to catch coding and billing errors.
- Train staff on payer-specific policies and requirements.
- Monitor denial trends to identify recurring issues and root causes.
Book a demo with CombineHealth to see our AI denial management software in action!
FAQs
What tools are available for managing denials in medical billing?
Healthcare organizations use denial management software, claim scrubbers, eligibility verification tools, and revenue cycle management (RCM) platforms to reduce and resolve denials. CombineHealth helps with end-to-end RCM tasks and denial management in medical billing.
How do denial rates vary among different insurance companies?
Denial rates vary significantly by payer due to differences in coverage policies, authorization requirements, and claims processing rules. Commercial insurers often have higher denial rates than Medicare, while rates can also vary by specialty, service type, and geographic region. Monitoring payer-specific denial trends helps identify problem areas.
What steps should I take if my Medicare claim is denied?
First, review the denial reason and any associated remark codes. Determine whether the issue involves eligibility, documentation, coding, or medical necessity. Correct claim errors and resubmit if appropriate. If you believe the denial is incorrect, follow Medicare's appeals process and provide supporting documentation.
Which medicare advantage plans deny the most claims?
Denial rates vary by Medicare Advantage organization and can change yearly. Some plans report higher prior authorization and payment denial rates than others, but performance differs across regions and service categories. Review CMS reports and plan-specific data rather than relying on broad rankings when evaluating denial patterns.
Where Can You Find a Comprehensive Denial Codes List?
Comprehensive denial code lists are available through the official X12 CARC (Claim Adjustment Reason Code) and RARC (Remittance Advice Remark Code) code sets. Additional resources include CMS publications, Medicare remittance advice guides, clearinghouse references, and payer-specific billing manuals that explain denial meanings and resolution steps.






