How to Improve Accounts Receivable Days in Medical Billing
Learn how to reduce Days in A/R in medical billing with benchmarks, DAR formula, and practical strategies to accelerate reimbursements.
March 7, 2026


Key Takeaways:
• Days in A/R measures how quickly healthcare providers convert delivered care into collected revenue. Lower A/R days signal efficient billing, while rising A/R often points to delays in documentation, claim submission, follow-ups, or denial management.
• High-performing organizations keep Gross Days in A/R under ~50 days and aim for 30–40 days. Strong clean-claim rates, faster claim submission, and proactive follow-ups are key drivers of better performance.
• Reducing A/R days starts with preventing rework. Improving first-pass resolution through better documentation, coding accuracy, and eligibility verification helps ensure claims are paid on the first submission.
• Operational discipline matters across the revenue cycle. Faster DOS-to-Drop, structured A/R follow-ups, and denial analytics help identify bottlenecks and resolve claims before they age into bad debt.
• AI and automation are increasingly helping organizations reduce A/R days. Tools that automate coding, denial detection, payer follow-ups, and revenue cycle analytics can accelerate collections and improve overall RCM efficiency.
In healthcare, revenue depends on how quickly the care you deliver turns into cash in the bank.
The answer lives inside your accounts receivable (A/R). Every claim waiting for adjudication, every unpaid patient balance, and every unresolved claim denial sits there—quietly tying up revenue that the organization has already earned.
But when the number of days the payment is stuck in the A/R begins to stretch, the effects ripple across the entire organization, and that’s exactly why Days in A/R is one of the most closely watched metrics in revenue cycle management.
In this article, we’ll break down what Accounts Receivable Days really measures, what AR Days benchmarks high-performing organizations target, and (most importantly) how to reduce it. We’ll also walk through practical AR management strategies across the revenue cycle, and real-world case studies where AI has shown significant impact on AR days for healthcare organizations.
What Is AR Days in Medical Billing?
Accounts Receivable (AR) Days measure the average number of days it takes for a healthcare provider to collect payment after a service is delivered. It reflects how long revenue stays in an unpaid or pending state before it is deposited into a healthcare organization’s accounts.
Example:
If a clinic submits a claim on January 1 and receives payment from the payer on February 10, that claim took 40 days to convert into cash. When averaged across all outstanding claims, this timeframe determines the organization’s overall AR Days.
What Makes AR Days a Crucial RCM Metric
AR Days is one of the most important revenue cycle management (RCM) performance indicators because it shows how efficiently a healthcare organization converts claims into cash.
Lower AR Days typically indicate faster reimbursements and smoother billing workflows, while higher AR Days suggest delays in claim processing, follow-ups, or payer payments.
AR Days also helps healthcare finance leaders and revenue cycle managers assess the effectiveness of their billing and collection strategies. Consistently rising AR Days may indicate underlying issues, such as:
- Delayed claim submissions
- Inefficient A/R follow-up processes
- Payer payment delays
- Unresolved claim denials
Recommended Reading: Common AR Scenarios and How to Address Them
What Factors Influence the 'Days in AR' in Healthcare Billing?
Days in A/R reflects the combined performance of multiple steps across the revenue cycle. These influences generally fall into two categories: internal operational factors and external payer or patient-related factors.
Internal Operational Factors Affecting Days in AR
Many drivers of A/R performance originate within the provider’s own workflows. This includes:
- Provider documentation delays: Claims cannot be submitted until encounter notes are completed and signed. Delayed documentation creates immediate bottlenecks in the billing pipeline.
- Inefficient billing workflows: Manual processes, outdated billing systems, or fragmented tools slow claim preparation and increase the risk of errors.
- Staffing or training gaps: Understaffed or inexperienced billing teams may struggle to keep up with claim follow-ups, denial resolution, and payer communications.
- Claim submission lag: Delays in submitting claims immediately extend the payment cycle. For example, submitting claims five days after a visit effectively adds five extra days before payers even begin processing.
- Claim denials: Coding errors, missing documentation, or incorrect patient information can lead to denials that require resubmission or appeals—adding weeks to the payment timeline.
External Factors Affecting Days in AR
Even when internal processes run smoothly, external variables outside the provider’s control can influence payment timelines. This includes:
- Payer mix and processing times: Different payers reimburse at different speeds. Medicare may process claims in about two weeks, while some commercial plans or HMOs can take significantly longer.
- Patient payment timelines: As patient responsibility grows with high-deductible plans, slow patient payments can extend the A/R cycle.
- Prior authorization requirements: Increasing prior authorization requirements can delay claim submission if approvals are pending or documentation is incomplete.
- Payer policy changes: Frequent updates to payer rules or billing requirements can lead to rework, compliance adjustments, or claim corrections.
How is AR Days Calculated in Medical Billing?
AR days is calculated using a simple formula that compares total outstanding receivables with the average amount billed per day.
The standard DAR formula in medical billing is:
This calculation estimates how many days it would take to collect all current receivables based on the organization’s current billing pace.
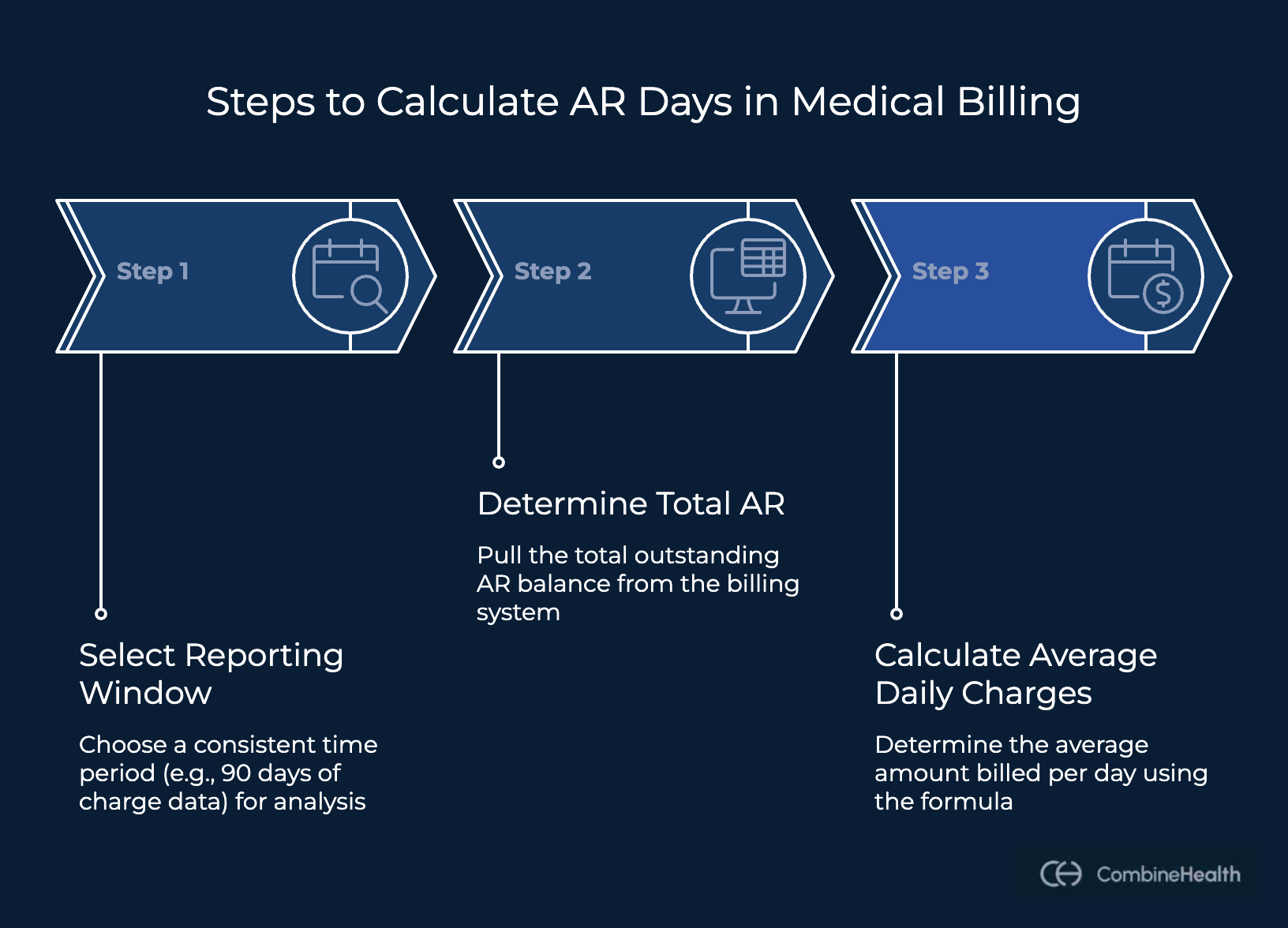
Here’s what the step-by-step Days in AR (DAR) calculation process looks like:
Step 1: Select a Reporting Window
Choose a consistent time period to analyze billing activity. Many healthcare organizations use 90 days of charge data to smooth out fluctuations in billing volume.
Step 2: Determine Total Accounts Receivable
Pull the total outstanding AR balance from your practice management or billing system as of the reporting date. This amount includes:
- Payer balances still pending reimbursement
- Patient responsibility balances that remain unpaid
Step 3: Calculate the Average Daily Charges
Next, determine how much the organization bills on an average day using this formula:
Alternative AR Days Calculation Method
Some organizations calculate AR Days using revenue instead of charges:
This method accounts for contractual adjustments and payer discounts, providing a closer representation of actual collectible revenue.
What’s A Good 'Days in AR' Benchmark for Healthcare Providers?
HFMA identifies 50 days or less as the acceptable benchmark for Gross Days in A/R for hospitals. Anything above this threshold typically signals inefficiencies in collections or revenue cycle workflows.
However, many healthcare organizations also track Net Days in A/R, which offers a more precise view of revenue cycle performance.
Within HFMA’s MAP benchmarking framework, Net Days in A/R typically ranges between 30 and 60 days, with high-performing organizations often keeping this metric closer to the lower end of the range.
Gross Days in A/R measures how long it takes to collect payments based on total charges billed before adjustments.
Net Days in A/R measures how long it takes to collect payments based on net patient service revenue after contractual adjustments and allowances.
However, evaluating A/R performance isn’t just about the overall number of AR days in your revenue cycle. HFMA also highlights the importance of A/R aging distribution, ensuring older receivables are tightly controlled.
Recommended thresholds include:
How to Reduce AR Days in Medical Billing
Follow these steps to reduce AR Days in your medical billing workflow:
1. Make "First-Pass Resolution" Your North Star
The fastest way to reduce AR Days is to ensure claims are correct the first time they are submitted, without edits, rework, or appeals.
First-Pass Resolution Rate (FPRR) refers to the percentage of claims that are successfully processed and paid by the payer on the initial submission.
When claims are processed the first time correctly, the revenue cycle moves much faster. Every denial or correction typically adds a minimum of 30 extra days to reimbursement timelines because staff must investigate the issue, correct the claim, and resubmit it.
Achieving a clean‑claim FPRR requires designing your revenue cycle around preventing errors before claims are submitted. And this typically involves making these proactive fixes to your revenue cycle:
Strengthening your CDI process
When clinical notes do not fully support the codes submitted, payers may reject the claim or request additional information.
Common clinical documentation issues include:
- Missing provider signatures
- Incomplete encounter notes
- Insufficient medical-necessity documentation
Some operational tactics to ensure clinical documentation integrity before claim submission:
- Standardize documentation templates for high-risk services
- Ensure templates capture key elements such as medical necessity, laterality, time, and complexity
- Conduct CDI audits focused on frequently denied services
- Provide quick-reference documentation guides for clinicians
Improving Medical Coding and Billing Accuracy
Mistakes such as incorrect CPT or ICD-10 codes, missing modifiers, or invalid code combinations often prevent claims from passing payer edits. And even when documentation and coding are correct, front-end data errors can still prevent claims from processing successfully.
Here’s how you can avoid these issues:
- Conduct pre-bill coding reviews for high-value or high-denial CPT codes
- Focus coder training on real denial trends rather than generic education
- Implement front-end claim edits for required fields and formatting
- Validate policy numbers, addresses, and identifiers before submission
CombineHealth’s Penny searches across CMS manuals, public payer policies, as well as uploaded PDFs (ex, insurance documents, provider’s contract with payers, etc.) to get insurance policy queries answered in seconds.
See Penny in Action
Performing Accurate Patient Eligibility Verification
Typical causes of patient eligibility-related errors include:
- Inactive insurance coverage
- Incorrect plan selection
- Coordination-of-benefits errors
Follow these operational tactics:
- Perform real-time electronic eligibility checks for every visit
- Reverify coverage before scheduled services
- Build payer-specific rules into patient registration workflows
.png)
2. Reduce Claim Submission Lag
The time between the Date of Service (DOS) and claim submission directly affects AR Days. Every day a claim waits before submission adds a full day to the revenue cycle before the payer even begins processing it.
Because this delay compounds downstream steps such as clearinghouse edits, payer adjudication, and patient billing, organizations track DOS-to-Drop as a core operational KPI.
Some actionable ways to reduce submission lag:
- Ensure same-day documentation: Encourage clinicians to complete and sign encounter notes on the day of service. If additional results are pending, finalize the visit and append addenda later rather than delaying charges.
- Move to daily charge capture: Submit claims daily instead of weekly. Use EHR work queues and end-of-day reconciliation by provider or department to ensure all encounters are captured.
- Track DOS-to-Drop as a KPI: Monitor submission lag by provider, department, and location. Review dashboards weekly and intervene quickly if the metric exceeds the 2–3 day target.
- Use alerts for stalled encounters: Set automated alerts for encounters older than 3 days without charges or provider signatures, allowing operations teams to clear bottlenecks before they translate into longer A/R cycles.
3. Implement Structured AR Management
Once claims are submitted, structured A/R management determines how quickly outstanding balances turn into cash. Here are some quintessential steps to follow:
Prioritize the Right Accounts
The most recoverable revenue typically sits in the 30–60 and 60–90 day buckets, where payer intervention can still resolve claims before they turn into bad debt
Follow these best practices:
- Segment work queues by aging bucket (0–30, 31–60, 61–90, 90+)
- Prioritize claims by balance size, payer type, and recovery likelihood
- Assign ownership for specific payer segments or aging buckets
CombineHealth’s Adam automatically checks claim status across payer portals and clearinghouse platforms and prioritizes claims based on age, dollar value, or payer rules.
Establish AR Follow-Up Cadence
Unstructured follow-ups often cause receivables to age unnecessarily. High-performing revenue cycle teams maintain a consistent follow-up rhythm until claims are resolved.
The recommended follow-up cadence is:
CombineHealth’s Adam makes AI-driven calls to insurers, navigating IVR systems or live agents to retrieve claim updates. The AI A/R follow-up solution also leaves voicemails and handles inbound calls when AR follow-up is required.
4. Monitor Aging and Enforce Accountability
A healthy A/R profile requires keeping older balances tightly controlled. Organizations typically aim to limit 90+ day balances to a small share of total A/R, since older receivables become increasingly difficult to collect.
Here are some best practices to monitor AR aging proactively:
- Review weekly aging reports by payer and denial reason
- Hold A/R huddles to identify root causes for claims exceeding 90 days
- Measure staff performance based on dollars resolved, not just activity metrics
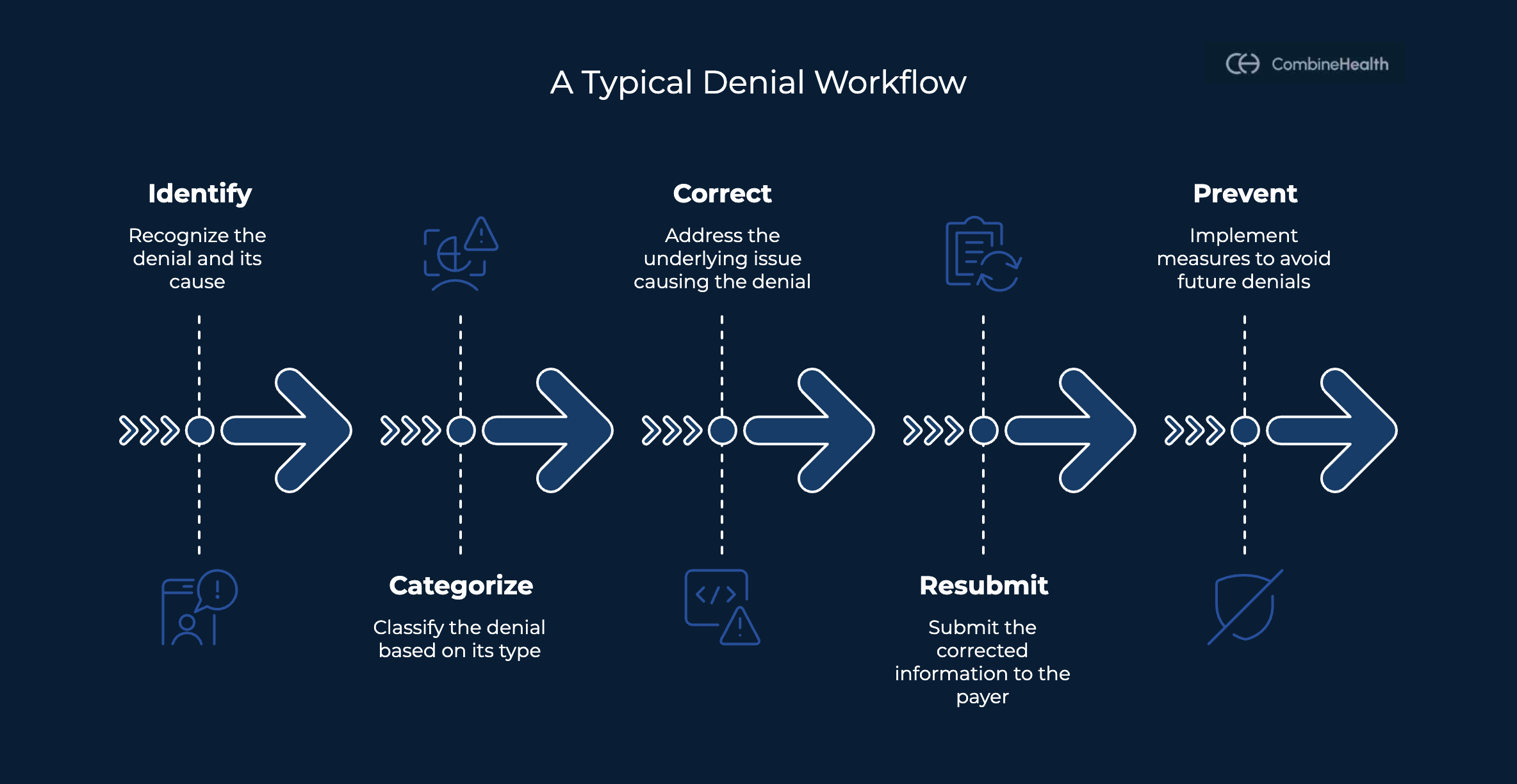
4. Invest in Good Denial Analytics
A data-driven denial analytics dashboard helps measure where denials occur, fix root causes, and prevent them from recurring. And AI and automation can significantly improve how organizations detect and process denials.
Ideally, a denial analytics dashboard should give revenue cycle leaders a clear, real-time view of where money is getting stuck and why.
At a minimum, it should show:
- Core denial performance metrics: Track key indicators such as denial rate, clean claim rate, first-pass resolution, denial resolution time, and Days in A/R to measure how efficiently claims move through the payment cycle.
- Denial breakdown by root cause: Analyze denials by payer, provider, location, procedure, and denial reason code to identify recurring patterns and pinpoint the operational areas driving denials.
- Operational activity visibility: Connect operational activity (claims created, claims submitted, follow-ups performed) with financial outcomes to see whether workflows are actually accelerating collections.
- Bottleneck detection across revenue cycle: Highlight where claims stall across the lifecycle, so teams can address delays early.
- Trend and pattern analysis: Surface changes in denial rates, payer behavior, coding distribution, or processing timelines to uncover systemic issues before they inflate A/R days.
CombineHealth’s Taylor helps add this intelligence layer to denial management by continuously analyzing the denial signals and surfacing insights automatically. One standout offering by Taylor is Conversational analytics, allowing revenue cycle leaders to simply ask questions such as:
- “What are the most common denial reasons requiring follow-up?”
- “How many payer calls were handled last week?”
- “How does this month’s E/M distribution compare to last month?”
.png)
Additional Accounts Receivable Metrics Healthcare Leaders Should Track
While Days in A/R is one of the most important revenue cycle indicators, CFOs and RCM leaders typically monitor several related metrics to understand why receivables are aging and where operational improvements are needed.
- Clean Claim Rate: The percentage of claims accepted by payers on the first submission without edits or rework.
- Net Collection Rate (NCR): The percentage of expected reimbursement actually collected after contractual adjustments.
- A/R Aging Distribution: Breaks down receivables into aging buckets (0–30, 31–60, 61–90, 90+ days) to track how balances accumulate over time.
- Denial Rate: The percentage of claims rejected by payers.
- Days to Pay: Days to Pay measures how quickly payers issue initial payment, while Days in A/R reflects the full reimbursement cycle, including follow-ups, secondary billing, and patient payments.
- DOS-to-Drop (Charge Lag): Measures the time between the Date of Service and claim submission.
How Does AI Help in Improving AR Days
Artificial intelligence is increasingly being used to remove manual bottlenecks across the revenue cycle. And real-world healthcare systems are already seeing measurable improvements:
HFMA Case Study – Auburn Community Hospital
Auburn Community Hospital, a 99-bed rural hospital, adopted AI across its revenue cycle to improve documentation accuracy and coding efficiency during the transition to ICD-10.
Using tools such as computer-assisted coding, natural language processing, and robotic process automation, the hospital enabled AI to analyze clinical documentation and suggest appropriate codes, allowing coders to work faster and focus on higher-value tasks.
Over time, this approach significantly improved operational efficiency:
- Discharged-not-final-billed (DNFB) cases dropped by 50%
- Coder productivity increased by over 40%
- Case-mix index rose by 4.6%.
All of these factors help accelerate claim submission and shorten the A/R timeline.
Intermountain Healthcare (AI Adoption Study)
Intermountain Healthcare implemented AI-driven analytics in its revenue cycle to reduce denials and accelerate reimbursements.
Using machine learning models trained on historical claims data, the health system identified patterns that typically led to denials and flagged high-risk claims before submission.
After integrating these tools into its billing workflows, Intermountain reported:
- A 15% reduction in Days in A/R
- A 25% decrease in claim denials within a year
Automating pre-bill reviews also reduced manual audits, allowing staff to focus on complex cases while improving billing efficiency and cash flow.
Turn Outstanding Claims Into Cash Faster
Reducing Days in A/R ultimately comes down to one question: how quickly can your team move unresolved claims toward payment? Even when claims are submitted correctly, a significant portion of revenue cycle work happens after submission—tracking claim status, resolving payer questions, and pushing stalled accounts toward resolution.
This is where dedicated A/R follow-up capacity becomes critical. CombineHealth’s AI-driven A/R agent, Adam, helps revenue cycle teams scale these efforts by automatically checking payer portals, navigating IVR systems, and retrieving claim status updates.
By prioritizing high-value claims and surfacing the next best action for each account, it enables teams to resolve outstanding balances faster while reducing the manual workload required to keep A/R moving.
Book a demo to see Adam in action!
FAQs
What tools are available for managing AR denial scenarios effectively?
Effective denial management typically combines claim scrubbers, payer rule engines, and denial analytics dashboards to detect issues early. Platforms like CombineHealth go further by pairing denial analytics with automated A/R follow-ups—analyzing denial patterns while AI agents check payer portals, call insurers, and prioritize high-value claims for faster resolution.
How can I improve AR learning scenarios for better billing accuracy?
Improve billing accuracy by strengthening documentation quality, implementing coding audits, analyzing denial patterns, and feeding those insights back into registration, coding, and authorization workflows. Regular staff training based on real denial trends—not generic refreshers—helps prevent repeat errors.
What is a good 'days in AR' benchmark for healthcare providers?
Industry benchmarks typically place gross Days in A/R at 50 days or less for hospitals. Many organizations operate around 45–60 days, while high-performing practices often maintain 30–40 days through efficient claim submission, strong denial prevention, and structured AR follow-ups.
Can you explain the 'DAR formula' used in medical billing?
The DAR (Days in Accounts Receivable) formula is:
DAR = Total Accounts Receivable ÷ Average Daily Charges.
It estimates how many days it would take to collect outstanding receivables based on the organization’s current billing volume.
What's the difference between gross and net days in AR?
Gross Days in AR uses total billed charges, while Net Days in AR adjusts for contractual allowances and calculates based on net patient revenue. Net AR provides a more accurate measure of collectible revenue and overall revenue cycle efficiency.
What factors influence the 'days in AR' in healthcare billing?
Days in AR is affected by claim accuracy, documentation delays, coding quality, claim submission speed, payer processing times, denial rates, patient payment timelines, and the effectiveness of AR follow-up workflows. Inefficiencies at any stage of the revenue cycle can extend AR timelines.






