AR Follow-Up in Medical Billing: How to Reduce Payment Delays in Healthcare
Improve AR follow-up in medical billing. Learn how automation, prioritization, and workflows reduce payment delays and boost healthcare collections.
Published on:
May 1, 2026

Key Takeaways:
• A/R follow-up in healthcare is where billed revenue turns into collected cash. If claims aren’t actively worked, they age out and become unrecoverable.
• Most A/R work in health systems today is manual and repetitive. Teams spend more time tracking claims than actually resolving them.
• Poor AR prioritization leads to missed revenue. High-value or time-sensitive claims often get buried in generic work queues.
• Claim denials are often symptoms of upstream issues in healthcare RCM. Without structured analysis, the same problems keep repeating across the cycle.
• Automation and AI help where work is repetitive, not where judgment is needed. It frees teams to focus on denials, appeals, and recovery instead of status checks
On any given Monday morning, an AR specialist opens a worklist with 60, 80, or sometimes 100 open claims.
Some are new.
Some have been sitting for 45 days.
A few are approaching filing deadlines.
None of them resolved themselves over the weekend.
That queue and what happens to it over the next few days is where most of the financial performance of a healthcare organization actually gets determined.
The HFMA considers A/R over 90 days a key indicator of revenue at risk, with well-performing organizations keeping this segment below 5%. And the way most organizations handle it today is still heavily manual, fragmented, and reactive.
That’s where the real problem begins.
This article looks at how A/R follow-up in healthcare really operates on the ground, why it consistently becomes a bottleneck, and where automation can realistically improve outcomes.
What is Accounts Receivable Follow-Up in Healthcare RCM?
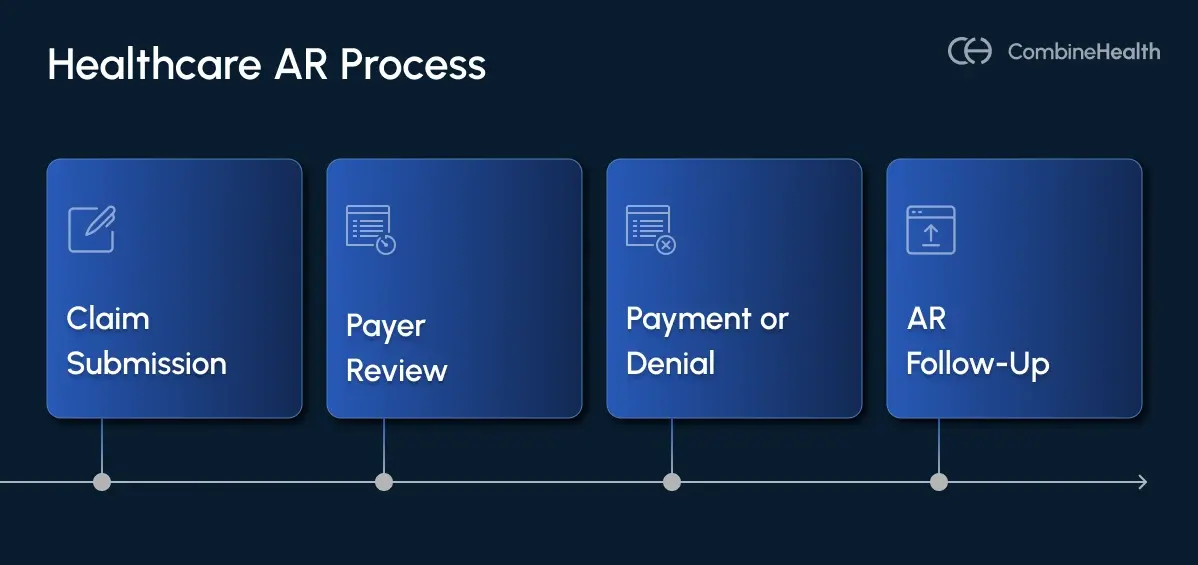
AR follow-up in healthcare is the systematic process of pursuing payment on insurance claims that haven't been resolved.
A claim goes out. The payer pays it, denies it, underpays it, or ignores it. AR follow-up handles everything that isn't a clean payment.
What makes it operationally demanding is that it's continuous, not episodic. This means AR teams aren't reviewing claims once and moving on. They're working daily aging queues, often returning to the same payer segments multiple times per week, by:
- Tracking claim status
- Making calls
- Documenting actions
- Deciding which balances to escalate, rework, or write off
Who Are the Stakeholders Involved in the AR Follow-up Process?
AR follow-up looks like a billing function from the outside, but it touches almost every part of the organization.
Internally, AR teams regularly pull in teams across different RCM functions, as required:
- Billing staff to correct and resubmit claims
- Coding teams to fix coding errors that caused denials
- CDI team to address documentation gaps
- Front desk teams to resolve eligibility and demographic issues
- Finance leadership when write-off decisions cross a dollar threshold
Externally, the AR follow-up function involves direct contact with payers through portals, phone calls, claim appeals submissions, and clearinghouses for claim status and rejection management. In some cases, the AR follow-up involves patients when balance responsibility shifts or coordination of benefits becomes part of the resolution path.
Importance of AR Follow-up in Medical Billing
AR follow-up is how billed revenue becomes collected cash. Without it, the rest of the healthcare RCM process doesn’t hold up.
When a claim goes unpaid, it doesn't stay recoverable forever. The older it gets, the harder it is to collect, and past a certain point, it becomes uncollectable entirely.
Here's why: payers set strict deadlines for claim resubmissions and appeals. Miss the window, and the claim is gone, regardless of whether the denial was legitimate. A claim that sat untouched for 90 days isn't just overdue, it may be unworkable.
A foolproof AR follow-up process prevents that from happening. It keeps someone actively monitoring every unpaid claim, working it before deadlines close, and catching underpayments or denials while there's still time to do something about them.
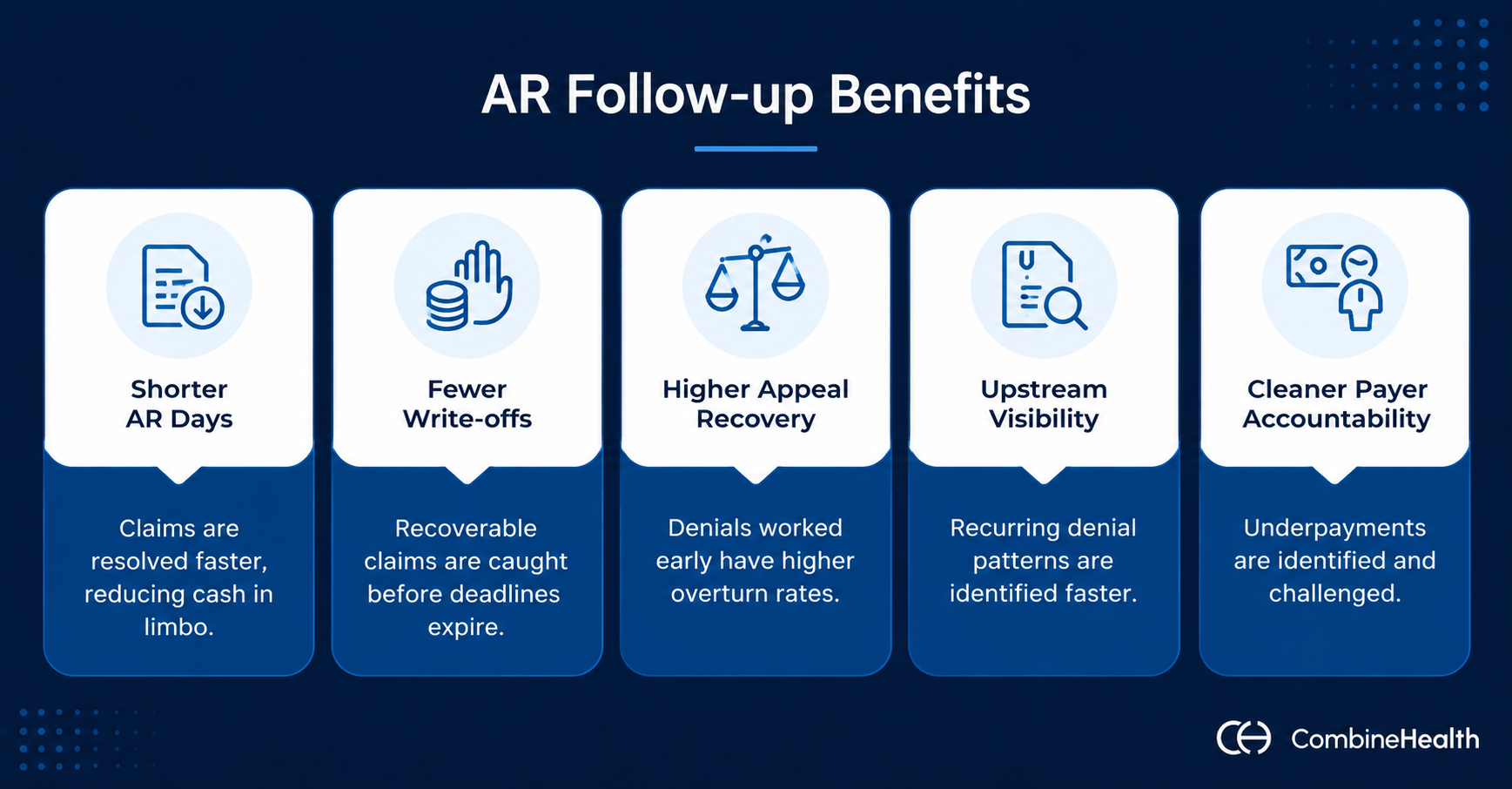
Done consistently, AR follow-up delivers compounding returns across the healthcare revenue cycle:
- Shorter AR days. Claims get worked and resolved faster, which means less cash sitting in limbo between service delivery and payment.
- Fewer write-offs. Recoverable claims get caught before filing deadlines expire, and balances age into bad debt.
- Higher appeal recovery. Denials worked early, with the right documentation, filed on time, overturn at significantly higher rates than ones that sit.
- Upstream visibility. Recurring denial patterns surface faster, giving coding and billing teams the information they need to stop the same errors from repeating.
- Cleaner payer accountability. Underpayments get identified and challenged instead of accepted by default.
AR Follow-Up Workflow in Healthcare (Step-by-Step Process)
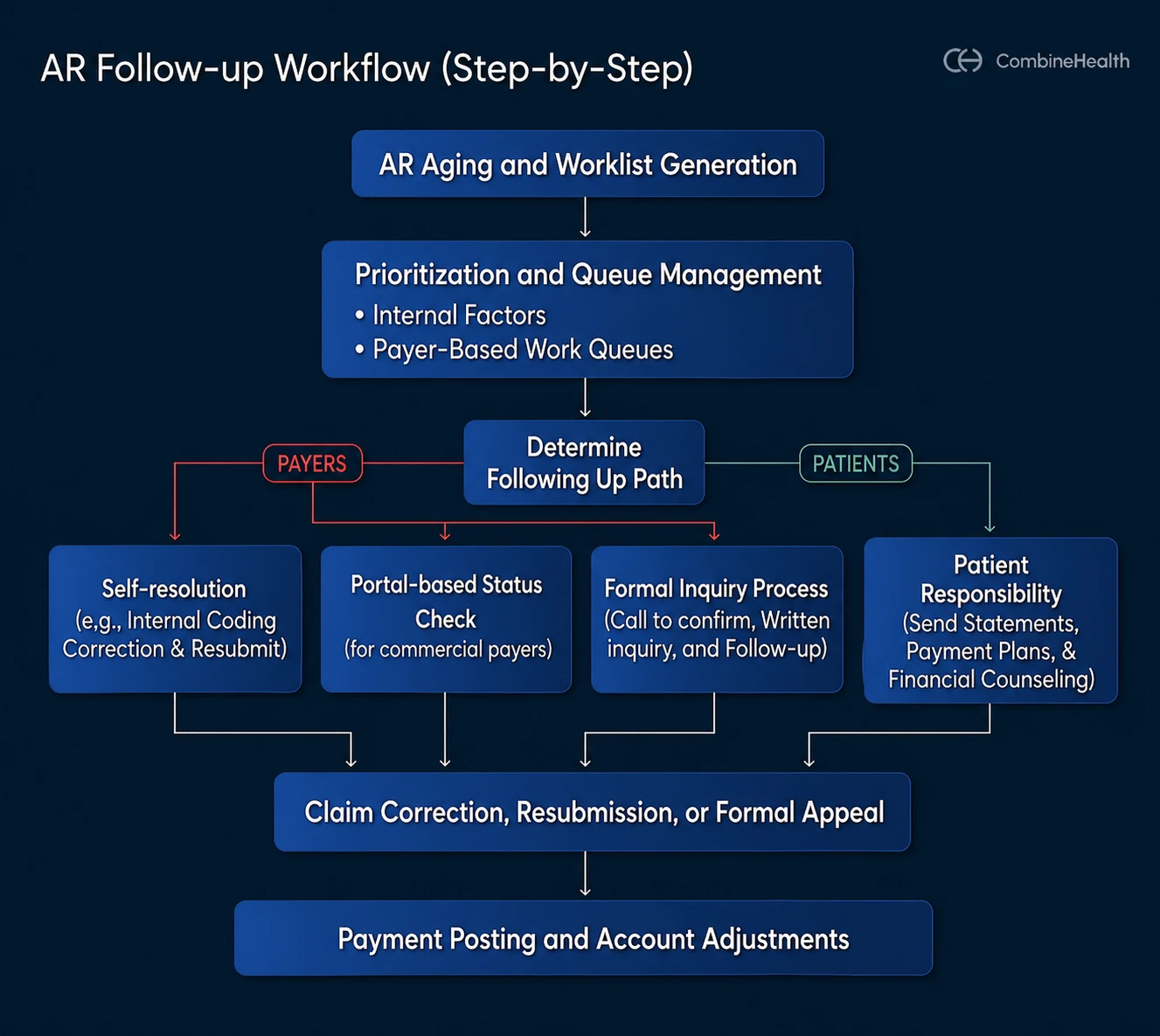
Here’s what the AR follow-up process looks like in a typical healthcare RCM setting:
1. AR Aging and Worklist Generation
Before anyone works a claim, the AR module or practice management system organizes outstanding balances into aging buckets and filters them by payer, financial class, balance size, and denial code.
Here’s what priorization based on AR aging buckets looks like (source: HFMA):
The output is a worklist: a prioritized queue of claims that need action.
Example:
A large orthopedic group might start the week with separate worklists for UnitedHealthcare commercial claims, Medicare, and Medicaid — each with different follow-up rules, portal requirements, and filing deadlines.
2. Prioritization and Assignment
Not every claim gets worked the same day. With hundreds of open balances across multiple payers, the difference between a well-run AR function and an overwhelmed one usually comes down to how the queue gets organized before anyone starts working it.
AR Prioritization happens across two dimensions: Internal claim factors and payer-based routing.
Internal Factors
Before a specialist touches a single claim, four internal characteristics determine which ones get worked first:
- Total charge. High-dollar claims move to the front. The financial exposure is highest, and the effort required to work them is often no greater than a low-balance claim.
- Aging bucket. Older claims are harder to collect. A claim at 75 days has fewer options than one at 35 — the resubmission window is narrower, the appeal deadline is closer, and payer responsiveness tends to decline with age. Claims approaching filing limits get treated as time-sensitive regardless of dollar value.
- Payer complexity. Some payers require significantly more effort per resolution — specific documentation formats, longer appeal timelines, and less predictable adjudication behavior. Government payers, Workers' Compensation, and auto liability claims fall into this category. Routing them to junior specialists without adequate experience typically results in missed deadlines and lost revenue. These queues belong to staff who know the rules.
- Denial complexity. The moment a denial is categorized, it should be routed to the right team. A medical necessity denial requires clinical documentation and a structured argument. A coding denial requires coordination with the coding team before anything gets resubmitted. Routing errors at this stage waste time and reduce overturn rates.
Payer-Based Work Queues
Beyond internal factors, claims are typically organized into dedicated queues by payer line of business:
- Medicare and Medicare Advantage Plans — Federal rules, strict timely filing limits, and plan-specific coverage policies that vary across MA carriers.
- Medicaid and State MCOs — State-by-state variation in billing rules, prior auth requirements, and appeals processes makes these queues among the most procedurally complex.
- Commercial payers (BCBS, Aetna, Cigna, UHC, Humana) — High claim volume, portal-heavy workflows, and contract-specific reimbursement rates that require underpayment monitoring alongside standard follow-up.
- Workers' Compensation and Auto Liability — Third-party liability cases with their own documentation requirements, adjuster contacts, and legal timelines. These are not standard insurance claims and should not be worked as if they are.
- Self-Pay and Patient Responsibility — Requires a different approach entirely: statements, payment reminders, financial counseling conversations, and in some cases, payment plan setup or referral to a collections partner.
3. Account Research and Root Cause Review
This is where the actual diagnostic work happens.
The AR specialist pulls details of the claim, such as:
- Claim history
- EDI acceptance reports
- ERA and EOB remarks
- Any prior notes on the account
Recommended Reading: How to interpret an ERA
The goal is to identify exactly why the claim is unresolved before taking any action.
Common checks include:
- Eligibility on the date of service
- Whether prior authorization was obtained and valid
- Coding and modifier accuracy
- Documentation sufficiency
- Whether the payer processed the claim according to contracted terms
Example:
A claim denied for CO-4 (procedure code inconsistent with modifier) points directly to a coding fix, not an appeal.
4. Following Up With the Right Owner
AR follow-up in healthcare happens across two different parties, each requiring a different process, different communication channels, and different resolution criteria:
- Payers
- Patients
For payers, AR follow-up involves checking claim status via EDI 276/277 transactions, payer portals, or direct provider service calls, and resolving missing information or clarifying denial reasons.
Recommended Reading: AR Scenarios in Medical Billing (With AR Calling Scripts)
The right way to approach payer follow-up depends on what the claim needs:
1. Self-resolution (no payer contact needed)
Some denials can be resolved without contacting the payer at all. A bundling denial, for example, is a coding issue first. The specialist checks whether the procedures are correctly bundled under current guidelines and whether an appropriate modifier exists to unbundle the service. If it does and the documentation supports it, the claim gets corrected and resubmitted internally.
2. Portal-based status check
For most commercial payers, the quickest way to check claim status is directly through the payer portal. Specialists log in, pull the claim, and get a current status without making a call. This is the default first step when portal access is available.
3. Formal inquiry process
When a claim requires direct payer contact — typically when a denial appears incorrect or information is insufficient — the process runs in two stages:
- Initial call: The specialist calls the payer to understand the denial reason and identify the correct inquiry channel. Most payers won't resolve anything over the phone — the call exists to confirm where to send the formal inquiry: a specific email address, fax number, or mailing address.
- Written inquiry: The formal inquiry, along with any supporting documentation, goes out through the payer's specified channel. Around 30 days later, the specialist follows up to confirm receipt and request an update.
For patients, AR follow-up means sending statements, payment reminders, or payment plan discussions when the balance responsibility has shifted to the patient's side.
5. Correction, Resubmission, or Appeal
Depending on what the research uncovered, the path forward is one of these things:
- If the claim was submitted incorrectly, the specialist coordinates with coding or registration to fix the error and resubmit.
- If the denial is disputable, an appeal is prepared with supporting documentation — clinical records, operative notes, coverage policies, or payer contract language.
Example:
A medical necessity denial from a commercial payer typically requires the physician's clinical notes alongside a written argument that the service met the payer's coverage criteria. A generic appeal letter without that documentation recovers at a fraction of the rate of one built around the specific claim.
6. Payment Posting and Adjustments
When payment arrives, it's often posted through ERA auto-posting and compared against the contracted rate. Any variance gets flagged for underpayment review.
Contractual write-offs, discounts, and bad debt adjustments are applied according to internal policy and approval thresholds. Write-offs above a certain dollar amount typically require a manager or director sign-off — a control that keeps recoverable balances from being adjusted off without a second review.
Challenges During AR Follow-up in Healthcare
If you talk to anyone managing A/R, you’ll hear the same thing: Besides reimbursement delays, they’re also dealing with a system that’s fundamentally working against them.
Let’s break down the challenges:
1. AR Follow-up Is Manual, Repetitive, and Never-Ending
A big chunk of the day of an AR specialist goes into things that don’t really move the needle:
- Logging into payer portals.
- Checking claim status.
- Copy-pasting updates into your system.
- Setting reminders.
Then, doing it all over again for the next claim.
And here’s the bigger issue:
This is high-effort, low-leverage work. Your most experienced A/R specialists aren’t solving complex denials — they’re stuck doing status checks, which eats up time that could’ve gone into actually resolving denials or recovering money.
And because it’s manual, it’s easy to miss things. One skipped follow-up, one wrong note, and the claim just sits there longer.
2. Teams Are Understaffed and Falling Behind
Even if you hire more people, it doesn’t solve the problem.
Because:
- Claim volumes keep increasing
- Denials are rising
- Payer requirements keep changing
So what happens?
Backlogs keep building. Aging buckets grow. Write-offs creep up.
3. AR Prioritization Is Often Guesswork
Not all claims are equal.
A $25K surgical claim sitting at 75 days in A/R should not be treated the same as a $120 office visit at 10 days.
But in many organizations, prioritization still depends on:
- Default work queues
- Payer-based sorting
- Or just “whatever is next in the list”
Without structured prioritization rules, teams aren’t working high-impact claims first — they’re just working what’s visible.
4. Critical Knowledge is Often Undocumented
Effective follow-up isn’t just about checking status.
It requires:
- Knowing payer-specific rules
- Understanding denial codes and appeal paths
- Tracking filing limits and escalation timelines
The problem is that most of this knowledge is undocumented, learned over time, or lost when someone leaves.
So every time there’s attrition, you’re losing operational intelligence.
5. The Tech Stack Is Fragmented
AR teams have to juggle not one but multiple systems, including:
- PMS
- EHR
- Clearinghouses
- Payer portals
- Spreadsheets
- Sometimes separate denial tools
Nothing is fully connected.
So you’re constantly switching tabs, re-entering data, and double-checking things, which increases the chances of mistakes.
6. Payer Updates Make Everything Harder
Even when your internal processes are solid, external friction remains:
- Payer portals change frequently
- Call center responses are inconsistent
- Policies are opaque and constantly evolving
- Appeal windows are shrinking
So A/R teams aren’t just managing claims, they’re also navigating unpredictability.
How AI and Automation Help Fix AR Follow-up Gaps
1. Automate Status Checks and Routine Follow-Ups
This involves repetitive and rule-based tasks such as:
- Logging into payer portals
- Checking claim status
- Updating notes
- Setting follow-up reminders
AI can:
- Retrieve claim status from payer portals or EDI feeds
- Capture denial codes and updates
- Trigger follow-up tasks when expected turnaround times are exceeded
Recommended Reading: Denial management in healthcare
2. Streamline Prioritization and Worklist Management
Traditional A/R workflows rely on static queues, often sorted by:
- Payer
- Aging
- System defaults
This approach does not always align with financial impact.
Automation and AI-driven models enable:
- Ranking claims based on value, aging, and recovery likelihood
- Identifying time-sensitive accounts approaching filing limits
- Surfacing patterns such as repeated denials from a specific payer
This creates dynamic worklists that direct attention to the most impactful claims first.
3. Build Denial Intelligence
A significant portion of A/R effectiveness depends on payer-specific knowledge.
Automation platforms can:
- Categorize denials systematically
- Link them to root causes (eligibility, documentation, coding, policy)
- Track outcomes of appeals and resubmissions
Recommended Reading: Top denial analytics vendors for health systems
4. Cross-System Coordination
A/R workflows typically span multiple systems, including:
- PMS and EHR
- Clearinghouses
- Payer portals
- Internal trackers
In the absence of full integration, staff act as the bridge between these systems.
Automation can:
- Move data between systems
- Update claim statuses across platforms
- Trigger downstream actions without manual intervention
5. Detection of Payer Trends and Policy Changes
Payer behavior is dynamic, and changes are not always communicated clearly.
Automation enables:
- Continuous monitoring of denial patterns
- Early identification of spikes tied to specific payers, codes, or locations
- Faster updates to workflows and rules based on observed trends
This shifts organizations from a reactive posture to a more responsive one, reducing the lag between issue emergence and corrective action.
Where Human Intervention Matters in AR Follow-Up?
Not all aspects of A/R follow-up are suitable for automation.
Areas that still require human expertise include:
- Complex clinical denials
- Interpretation of medical necessity criteria
- Nuanced appeal writing
- Judgment-based escalation decisions
Automation is most effective when it supports these activities.
Recommended Reading: Top AR Follow-up Services in the US for Health Systems
Key AR Metrics to Track in Healthcare
These nine metrics give AR teams and finance leaders a complete picture of follow-up performance — where cash is moving, where it's stalling, and where it's quietly disappearing.
1. Days in AR
Days in AR measures the average number of days between delivering a service and collecting payment for it, calculated as total AR divided by average daily net charges.
When this number climbs, it usually means one of three things: follow-up is slow, denial volume is high, or payers are delaying. MGMA benchmarks put the general target under 40 days, with top performers landing between 30 and 35, depending on specialty and payer mix.
2. AR Aging and Percentage of AR Over 90 Days
Days in AR tells you how fast you're collecting on average. AR aging tells you where the problem is concentrated. Claims are distributed across aging buckets — 0 to 30 days, 31 to 60, 61 to 90, 91 to 120, and beyond — and the percentage sitting past 90 days is the number to watch most closely.
A high share of AR in older buckets is a direct signal of unresolved denials, missed filing deadlines, or follow-up that isn't keeping pace with claim volume. HFMA flags AR over 90 days as a core measure of AR health.
3. Net Collection Rate
Where Days in AR measures speed, net collection rate measures completeness. It tracks how much of your allowable revenue (charges minus contractual adjustments) you actually collect after denials, write-offs, and underpayments are accounted for.
A net collection rate below 90% means revenue that was legitimately owed is leaving through denials that weren't appealed, underpayments that weren't caught, or balances that aged into write-offs. Healthy organizations operate at 90 to 95% and above. Anything materially lower is a systemic leakage problem, not a one-off.
4. Initial Denial Rate
Initial denial rate is the percentage of claims denied on first submission. It’s the upstream quality indicator that the AR queue makes visible — high denial rates mean eligibility, authorization, coding, or documentation problems are making it past submission without being caught.
5. First-Pass Acceptance Rate (Clean Claim Rate)
The percentage of claims paid or accepted by the payer on first submission, with no edits or denials required. This is the leading indicator that tells you how well the front end of the revenue cycle is performing before problems reach the AR queue.
6. Follow-Up Success Rate
This metric specifically measures AR team effectiveness: resolved claims divided by claims worked, per period or per specialist. It answers a question that denial rate and AR days don't: when the team actually touches a claim, how often does that touch result in resolution?
A high claim volume with a low follow-up success rate means activity is happening without outcomes.
7. Appeal Success Rate
This is equal to appeals overturned divided by total appeals submitted.
This metric surfaces two distinct problems depending on which direction it fails. A low overturn rate on a high appeal volume usually means the team is appealing everything regardless of merit, diluting effort across unwinnable cases. A low overturn rate on a selective appeal volume usually means the appeal content or documentation isn't making the case effectively.
8. Bad Debt Ratio
Bad debt write-offs as a percentage of total service revenue. This is the final accounting of what didn't get collected after all AR and collection efforts concluded — and it's heavily influenced by what happened at the very beginning of the encounter, specifically eligibility verification and financial clearance.
9. Payer Performance Scorecard
Each of the metrics above can and should be tracked by individual payer — average Days in AR, denial rate, underpayment variance from contract, and percentage of AR over 90 days — broken out per payer rather than aggregated across the book.
The aggregate numbers tell you what's happening across your AR. The payer-level breakdown tells you who is causing it.
Your AR Team isn’t The Problem—It’s How the Workflow is Set Up!
If you step back, most A/R teams aren’t underperforming. They’re just working inside a system that makes it hard to win.
Too much of the day goes into:
- Checking status
- Moving between systems
- Figuring out what to work next
- Dealing with the same issues again and again
And when that’s the case, even a strong team will fall behind.
What actually changes outcomes is how you structure the work, so AR follow-up doesn’t depend on memory, important claims do not get buried in queues, and your AR team spends their time solving issues, not tracking them.
If you’re trying to improve A/R performance, our AI AR management solution can help.
Book a demo to see how this can look in practice — what gets automated, what stays manual, and how teams actually work differently!
FAQs
Where does AR Follow-up fit in the healthcare revenue cycle?
AR follow-up sits after claim submission in the revenue cycle. Once a claim is billed, any unpaid, denied, or underpaid balance moves into A/R. Follow-up ensures those claims are tracked, corrected, appealed, and ultimately converted into collected revenue.
What do AR teams do on a day-to-day basis?
AR teams review aging reports, check claim status, contact payers, investigate denials, correct errors, resubmit claims, and file appeals. They also document actions, track follow-up dates, and coordinate with coding, billing, and front-end teams to resolve issues preventing payment.
Why AR follow-up in healthcare matters?
AR follow-up directly impacts cash flow. Without it, unpaid claims age, appeal deadlines are missed, and revenue is lost. Timely follow-up improves collections, reduces write-offs, increases denial recovery, and provides visibility into upstream issues affecting billing accuracy and reimbursement.
What are the key components of healthcare AR follow-up?
Core components include claim prioritization, account research, denial analysis, payer communication, correction or appeal, and follow-up tracking. It also involves documentation, coordination with internal teams, and monitoring deadlines to ensure claims are resolved before filing limits expire.
What are the standard AR follow-up timelines?
AR follow-up typically starts within 7–14 days of claim submission. Claims are monitored across aging buckets (0–30, 31–60, 61–90, 90+ days). High-risk claims nearing filing limits require immediate action. Regular follow-ups continue until payment, resolution, or write-off.
What are the strategies for effective AR follow-up for healthcare billing teams?
Effective strategies include prioritizing high-value and time-sensitive claims, using denial analytics to identify root causes, maintaining consistent follow-up schedules, standardizing workflows, and ensuring strong coordination across teams. Increasingly, teams use automation to reduce manual work and improve follow-up consistency.






