When Point Solutions in Healthcare RCM Fail
Point solutions fix symptoms. RCM demands a cure. Learn when to move beyond fragmented tools—and what to look for in an end-to-end AI RCM platform.
Published on:
March 16, 2026


Key Takeaways:
• Point solutions shine in specific, contained problems—a coding backlog in one specialty, an acute staffing crisis—but struggle the moment RCM complexity expands beyond that narrow scope.
• Most RCM problems originate upstream, but point tools are anchored downstream, which means you're often fixing the symptom while the root cause keeps generating new ones.
• The more vendors you add, the more fragmented your data, accountability, and workflows become—and the harder it gets to draw a straight line from technology investment to revenue outcome.
• Evaluating an end-to-end platform means going beyond features: ask who owns integration, whether AI is truly explainable, and whether the solution can grow with your organization's strategy.
• The real cost of point solutions compounds over time — in hidden integration work, training overhead, and the organizational bandwidth consumed by managing a stack that was never designed to work together.
If you work in healthcare revenue cycle, you've probably thought like this at some point:
- A coding backlog appears? Let’s bring in a specialized coding tool.
- Denials start climbing! A denials management solution to the rescue.
- Prior authorizations become a bottleneck? Oh, there's a tool for that too!
Each decision makes sense in the moment—you saw a real problem, found a focused fix, which brought you a quick win.
And then one fine day, you look up and realize you're managing half a dozen vendors, each with their own dashboard, their own logic, and their own definition of what "performance" means.
Turns out, this is one of the most common stories in healthcare revenue cycle today.
A 2025 survey of 600 US healthcare revenue cycle, finance, and technology leaders found that just over 70% of organizations use one or two software vendors to manage all aspects of RCM—and about 20% use three to four.
Across the industry, point solutions have become the default response to RCM complexity—purpose-built tools for different stages of RCM, each promising to solve one piece of the puzzle better than anyone else.
Sometimes they deliver. But more often, the puzzle doesn't get any easier to solve—it just adds more pieces.
This article is an honest take on when point solutions in healthcare RCM work, when they don't, and when it’s time to look for an end-to-end RCM solution.
Scenarios When They Might Actually Be a Good Fit
Let's be honest about something: point solutions aren't inherently broken. In the right conditions, they can be genuinely impressive—and pretending otherwise would miss the point entirely.
Here's where they actually shine:
- High-volume, well-defined workflows: Case studies from many point solutions show that autonomous medical coding is most mature in high-volume specialties like radiology and emergency.
- Acute staffing crises: When you're staring down hundreds of uncoded charts, and your coding team is already stretched thin, a point solution that drops into the mid-cycle within days is a lifeline.
Verdict: If your core problem is a coding backlog in one or two specialties and your upstream/downstream RCM is otherwise healthy, a point medical coding solution can be a quick win.
When It’s Probably Time to Look The Other Way
Point solutions are good at solving the problems you can see. The trouble is, most RCM problems aren't where they appear to be.
Denials are a classic example.
Since they show up at the back end (a claim rejected, a payment delayed, a write-off taken), the instinct is to buy a denials tool.
But the real problem is everything upstream, i.e., a documentation gap, an eligibility miss, a coding inconsistency nobody caught because no single system was watching the whole journey.
So, if you’ve been considering any of the following notions lately, it’s probably time you started exploring end-to-end AI RCM solutions:
You Want To Look at the Root Cause, Not Just One Symptom
Buying a tool for every symptom doesn't fix the disease—it just gives you more dashboards showing how sick your workflows are.
Every point solution is optimized for its own metric: coding turnaround time, denial overturn rate, and clean claim percentage. But those metrics don't talk to each other, and neither do the tools behind them.
For instance, most organizations treat denials as a back-end clean-up function—a denial arrives, someone works it, and an appeal goes out. The cycle repeats.
What rarely happens is a serious investigation into why the denial showed up in the first place:
- A documentation gap at the point of care?
- A coding inconsistency?
- An eligibility issue that slipped through intake?
- A payer rule that changed last quarter?
That’s the difference between a point solution that just responds to a denial and a system that works toward preventing denials altogether.
CombineHealth's denial management suite does exactly that!
We deploy a set of AI agents that each own a specific part of the problem: payer policy review, coding and documentation audits, eligibility validation, appeals drafting, and analytics.
Crucially, these AI agents work in concert.
When a denial lands, coding validation, policy review, AR follow-up, and the claim appeals process happens autonomously. And because the same system is scanning claims before submission to find documentation gaps, coding inconsistencies, and other issues, many of those denials never happen at all.
You’re Way Too Busy To Deal With Fragmented Data
The more point solutions you add to your stack, the more complex managing them gets. In fact, organizations using multiple RCM solutions actually reported more denial trouble, not less. Here’s why that happens:
- Every vendor is another integration project: When payers change policies, every impacted tool needs to be updated, tested, and redeployed.
- Another login, another queue, another dashboard: Context-switching doesn't just slow people down. For coders, billers, and denial specialists already running at capacity, it's a direct contributor to burnout and error.
- No accountability, whatsoever: When AR starts climbing, and nobody can agree on why, accountability diffuses across the stack. Each system tells a different story. No one owns the outcome.
The underlying problem is that most point solutions weren't designed to share context—they were designed to solve their own problem cleanly and hand off.
Data interoperability is what breaks that cycle, but only if it's built in from the start, not bolted on after the fact.
CombineHealth connects directly into your existing EHR and Practice Management systems using HL7 and FHIR standards, which means your current infrastructure stays intact.
There's no rip-and-replace, no months-long implementation runway, and no parallel system to manage while you wait for value to show up. Your existing stack becomes the foundation—and for the first time, it actually behaves like one.
You’re Looking to Resolve Upstream Issues, and Not Just One Metric
The denial you're fighting today was created weeks ago, and your point solution wasn't there to catch it.
That’s because most denial and revenue leakage problems start upstream—the point when that laterality was missed in the documentation, or a generic code like "unspecified fracture of femur" was used instead of indicating whether it is the shaft, distal, or proximal end.
The problem is most point tools often anchor on a single KPI (e.g., denial overturn rate, coding turnaround time) without closing the loop. This is why breakdowns in eligibility, pre-authorizations, documentation, coding, and billing cascade into each other in ways that no single-metric tool is built to trace. By the time the denial surfaces, the window to fix the root cause has long passed.
What actually moves the needle is catching those gaps before the claim ever leaves the building. That means having intelligence embedded at the documentation layer that:
- Reads clinical notes in context
- Flags missing specificity
- Identifies coding inconsistencies
- Raises the right questions with providers while there's still time to act
CombineHealth's approach centers this kind of upstream intelligence in Amy, an AI agent built for coding and CDI.
Beyond assigning accurate ICD-10 and CPT codes, Amy flags documentation gaps as she works— vague diagnoses, missing laterality, under-coded complexity—and raises compliant queries to providers when clarification is needed.
She also tracks CDI issues across charts and providers over time, surfacing patterns like recurring documentation gaps by physician or service line that no human reviewer would catch consistently at scale.
You Lack the Bandwidth to Evaluate and Implement Multiple Solutions
Most RCM and IT teams are already at their limit, and every new point solution adds to the load, not reduces it.
Each new tool brings its own implementation cycle, training program, super-user development, and change management burden. That work lands on the same teams already managing denials, payer escalations, and staffing gaps. And when hospitals are sprawling multiple IT vendors, they instead slow down operations due to:
- Duplicated functionality
- Training fatigue
- Integration work that distracts from strategic initiatives
And the economics, over time, rarely favor the point solution path.
When you add implementation, integration, ongoing maintenance, super-user development, and the compounding change management burden across a growing stack, the "cheaper" option can quietly become the more expensive one. Three to five years in, many organizations find they've paid for transformation and received incremental improvement.
How to Evaluate an End-To-End AI RCM Vendor for HealthCare?
Choosing an end-to-end RCM vendor is a different kind of decision than buying a point solution. For a point solution, you typically ask: Does it solve this specific problem well? But, with an end-to-end RCM solution, you evaluate if it fits where you’re actually trying to go.
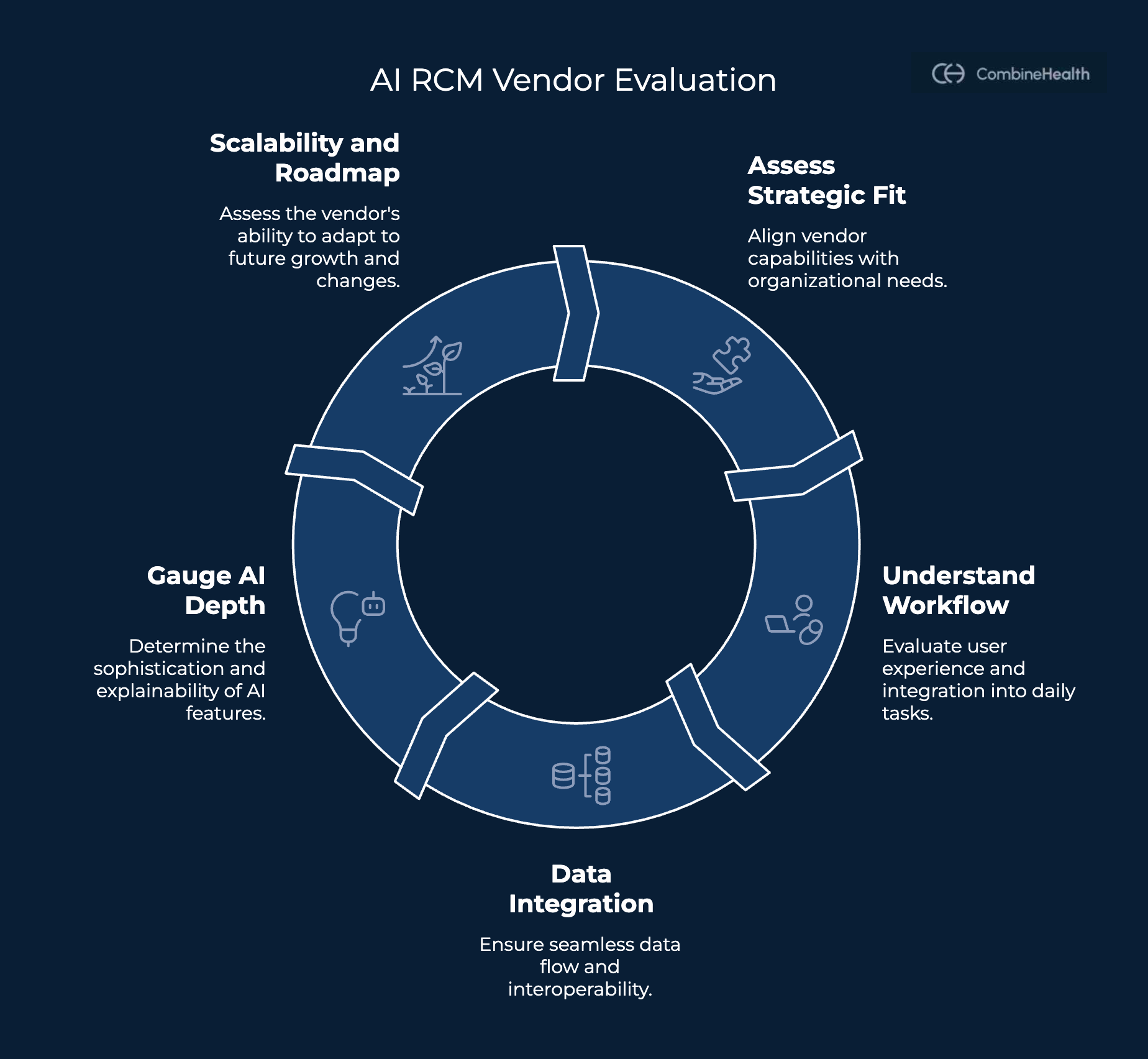
Here's what to look for:
Look for Strategic Fit
Most organizations have a sense of their biggest pain points—denials, coding backlogs, slow AR—but fewer have traced those problems back to their origin. That's the conversation to have first, because the right vendor depends entirely on where in the cycle your revenue leaks from.
The critical question is whether the vendor you're evaluating can actually touch the root causes of your revenue leakage—or whether they're just very good at one symptom.
Understand the Workflow and User Experience
A platform can have the most sophisticated AI in the market and still fail if your teams can't work in it without friction.
Workflow fit isn't a secondary consideration—it's often the difference between AI that transforms RCM performance and one that gets quietly abandoned six months post-implementation.
The honest version of this evaluation starts with your frontline staff. Coders, billers, denial specialists, and front-desk teams each have their own daily rhythm—and the question worth asking is whether a new platform fits that rhythm or disrupts it.
A few questions worth pressure-testing before you commit:
- How many logins, dashboards, and queues will staff need to manage daily?
- Does the solution integrate into how your teams actually work?
- How much change management does this realistically require?
- Will the staff be toggling between systems with different rules and different definitions, and standardization?
Assess Data Integration and Interoperability
A platform is only as good as its ability to connect with the systems you already rely on.
Start with the integration question, and be specific about who owns it. Most vendors will tell you they integrate with Epic, athenahealth, MEDITECH, and every major clearinghouse. What they're less forthcoming about is how much of that integration work lands on your IT team, and what the ongoing maintenance looks like when things change—and in healthcare, things always change.
Ask these questions:
- Does data from this platform flow into a single source of truth, or does it create another silo?
- Who owns making the integration work in practice?
- Does the platform give you visibility across the full revenue cycle or just your slice of it?
Gauge the AI and Automation Depth
Not all AI in RCM is created equal, and the gap between a rules-based workflow engine and a genuinely adaptive AI system matters more than most vendor conversations let on.
The first question to ask is a simple one: Is this actually AI, or is it automation dressed up in AI language?
Rules-based systems follow fixed logic—if this, then that. They're useful, but they don't learn. They don't adapt when a payer quietly changes their adjudication behavior, or when a new physician joins your group with documentation patterns the system has never seen.
Real AI and machine learning improve over time, trained on your own data—your denial patterns, your coding history, your payer contracts—and get more accurate the longer it operates in your environment.
The second question is more important: can the system explain what it's doing and why?
When AI decisions can't explain themselves, the liability doesn't disappear — it lands on your balance sheet. A few reasons this matters in practice:
- You own the risk, even when AI makes the decision.
- Explainability enables oversight at scale.
- It shifts RCM from reactive to preventive.
The vendors worth evaluating are those who can show you both: AI that learns from your specific environment, and explainability that lets your teams understand, trust, and act on what it surfaces.
Recommended Reading: Explainable AI in Healthcare
Understand the Scalability and Roadmap
The scalability question is straightforward but often underasked: what happens when you add a new location, acquire a practice, expand into a new service line, or shift toward value-based contracts?
With a point solution, the honest answer is usually "we'll figure it out then" — which typically means another procurement cycle, another integration project, and another vendor to manage.
The deeper question is about strategic flexibility. RCM doesn't stand still—payer mixes shift, contract models change, and acquisitions happen.
A solution that fits your current operating model but can't adapt to a different one will eventually become an obstacle. Before you commit, it's worth asking: If our strategy changes significantly in three years, does this solution flex with us, or do we start over?
Is Your RCM Stack Working For You or Against You?
Point solutions solve problems. Platforms build leverage. If you've read this far, you already know which one your organization needs.
CombineHealth is the end-to-end RCM platform built for health systems ready to stop patching and start compounding. Let us show you what that looks like.






