Utilization Management: What Healthcare Providers Need to Know About Payer Coverage Decisions
A practical guide to utilization management in healthcare, covering payer coverage decisions, prior authorization, denials, concurrent review, and strategies to reduce revenue cycle disruptions.
Published on:
May 7, 2026


Key Takeaways:
• Utilization management is the set of payer-side processes that decide what services get covered, when, and at what level.
• UM applies at three checkpoints in the revenue cycle: before care (prior auth, eligibility), during care (concurrent reviews), and after care (retrospective audits).
• Most UM-related denials start upstream—at scheduling, documentation, or policy alignment—meaning downstream claims cleanup can't recover what was lost earlier.
• AI agents that automate eligibility verification, surface documentation gaps in real time, and monitor payer policy can reduce UM-related denials and free teams from routine compliance work.
Prior authorization denials, level-of-care downgrades, and medical necessity rejections show up on nearly every hospital's denial report. That stack of at-risk revenue has one name behind it—utilization management.
Hospitals spent $43 billion in 2025 trying to collect payments insurers owed for care already delivered, according to the American Hospital Association. A significant share traces back to UM-related denials, downgrades, and authorization gaps.
Understanding utilization management at a much deeper level helps RCM teams stop those denials at the source instead of fighting them after the fact.
This guide breaks utilization management down phase by phase—what it is, who actually owns it in a healthcare RCM team, how it fits into your revenue cycle, and where your team can move the needle.
What Is Utilization Management in Healthcare?
Utilization management is the set of processes a payer uses to decide whether they will cover a service, at what level, and under what conditions—before, during, or after a healthcare service is delivered.
At its core, utilization management is a cost-control mechanism set by payers. Health plans, Medicare Advantage organizations, Medicaid managed care plans, and self-insured employers often work with third-party vendors like Carelon, eviCore, or Magellan to review care requests. They evaluate each requested service against medical necessity criteria and decide what they’ll pay for.
Payers design the rules and make the decisions. Providers do the work of complying, which includes:
- Submitting prior authorizations
- Defending medical necessity
- Navigating concurrent reviews
- Pushing back on retrospective audits that consume staff time and drive denials when handled poorly
The Purpose of Utilization Management in Healthcare
Two purposes drive how payers design UM programs: cost containment and ensuring care is delivered appropriately.
Cost Containment
Utilization management is the payer's primary lever for controlling spend. Without checks, payers argue, expensive or unnecessary care would erode benefit dollars and push premiums up across the risk pool.
Prior authorization, step therapy, and concurrent review all fall under this rationale—keep care within evidence-supported, cost-effective bounds.
Medical Necessity
Utilization management in healthcare also exists to ensure healthcare services:
- Meet clinical guidelines
- Are delivered at the right level of care
- Don't duplicate care the patient already received
Example:
A high-cost imaging order is reviewed against criteria that ask: was conservative therapy tried first? Are symptoms severe enough to warrant the test? Is there a less expensive alternative that should be ruled out first?
Note:
In practice, cost containment and medical necessity blur.
For example, a denial labeled "not medically necessary" is also, by definition, a denial that saves the payer money. Providers often experience utilization management primarily as a cost-control mechanism, even when payer documentation cites clinical rationale.
Who Actually Performs Utilization Management?
Utilization management has stakeholders on both sides of the desk. The clearest way to describe it is to separate who decides from who responds.
1) On the Payer Side: Where the Decisions Happen
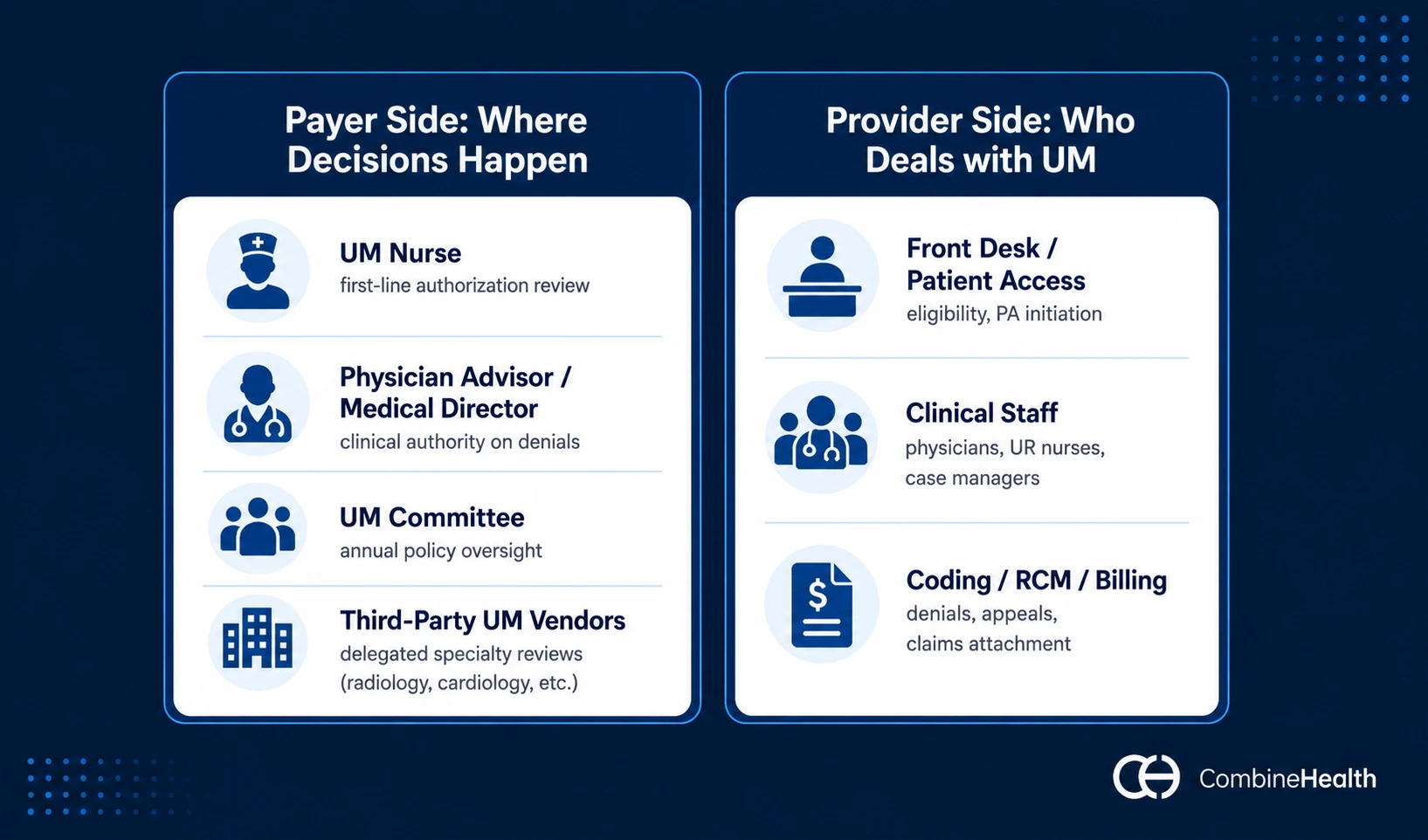
The payers' utilization management team typically includes:
- Utilization management nurse/utilization review nurse: typically a registered nurse trained in utilization management criteria like InterQual or MCG. Reviews authorization requests against clinical guidelines and approves straightforward cases. The frontline of payer-side UM.
- Physician advisor/medical director: handles complex cases, peer-to-peer reviews, and final clinical authority on denials. UM nurses cannot deny on clinical grounds—only a physician reviewer can.
- UM committee: for Medicare Advantage plans, CMS now requires an internal committee that reviews UM policies annually for alignment with Traditional Medicare coverage rules.
- Third-party UM vendors: many plans delegate utilization management for specific service lines to outside vendors. Examples include Carelon Medical Benefits Management and eviCore (for radiology, cardiology, and other specialty utilization management). BCBS plans across multiple states delegate to these vendors regularly.
2) On the Provider Side: Who Deals With Utilization Management
UM responsibilities on the provider side cut across three role groups, each handling a different slice of the compliance work:
- Front desk/patient access: eligibility and benefits verification, identifying which services need prior authorization, initiating auth requests, and flagging UM issues at scheduling. This is the front line where most authorization-related denials are either prevented or set in motion.
- Clinical staff (physicians, UR nurses, hospital case managers): generating clinical rationale, documenting medical necessity, responding to payer requests for additional information, and conducting peer-to-peer reviews. Their documentation is what makes or breaks medical necessity decisions on both prospective and concurrent reviews.
- Coding, RCM, and billing teams: attaching authorization numbers to claims, working denials tied to UM, and building and submitting appeals. These are the teams whose workload is most directly inflated when something goes wrong upstream.
The handoffs between these three groups are where revenue leaks for providers, such as a missing authorization number at billing, documentation that didn't get to the utilization management nurse in time, or a denial that nobody routed to appeals.
Recommended reading: Best practices for revenue integrity in healthcare
How Utilization Management Fits Into the Revenue Cycle
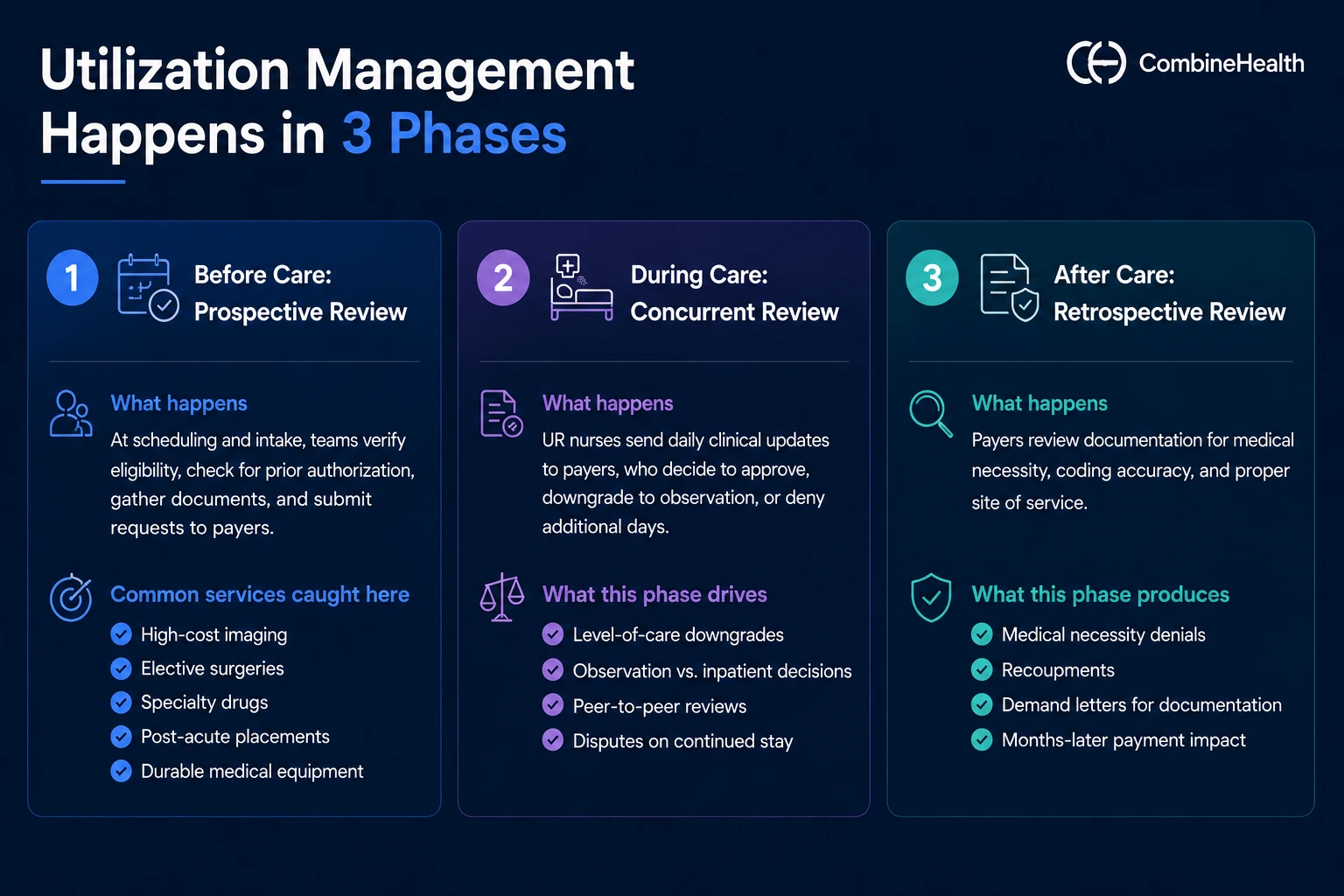
Utilization management touches three distinct phases of RCM, each one mapping to a different type of UM review:
Before Care: Prospective Review
This is where UM most often appears for the first time. Prospective review (also called pre-service review) happens before care is delivered. It includes prior authorization, precertification, predetermination, and step therapy.
For providers, this phase shows up at scheduling and intake. Patient access teams verify eligibility, check whether the planned service requires prior authorization, gather supporting documentation, and submit requests through payer portals or electronic transactions.
The most common services caught here: high-cost imaging, elective surgeries, specialty drugs, post-acute placements, and durable medical equipment.
During Care: Concurrent Review
Once a patient is admitted, utilization management in healthcare continues as concurrent review (sometimes called continued-stay review). Hospital UR nurses send daily clinical updates to the payer, who decides whether to keep approving the inpatient level of care, downgrade to observation, or deny additional days.
This phase is where level-of-care downgrades happen—the payer decides Day 3 should have been observation rather than inpatient, and reduces payment accordingly. It's also where peer-to-peer reviews get triggered when the hospital and payer disagree on continued stay.
After Care: Retrospective Review
Retrospective review happens after care is delivered, often as a post-payment audit. The payer reviews documentation to determine whether services were medically necessary, properly coded, and delivered in the right setting.
This is the phase that produces medical necessity denials, recoupments, and demand letters for additional documentation—sometimes months after the patient is discharged. It's also where a strong clinical documentation improvement software can do the most defensive work.
Example:
To simplify this, let’s take a planned total knee replacement for a Medicare Advantage patient:
- Prospective: The orthopedic team submits a prior authorization, gets approval, and proceeds with surgery.
- Concurrent: During the inpatient stay, hospital UR nurses send daily updates to the payer, who challenges the Day 2 inpatient status. A peer-to-peer reverses the challenge.
- Retrospective: Two months later, the payer's audit team requests the full medical record, questioning the medical necessity of one inpatient day. The hospital's denials team appeals and recovers the payment after a 60-day cycle.
How Utilization Management in Healthcare Differs From Medical Billing or Claims Processing
Utilization management is upstream. Medical billing and claims processing are downstream.
UM determines whether a service is covered and authorized. Medical billing translates the rendered service into a claim. Claims processing (or adjudication) is the payer's process of evaluating that claim against benefits, coding rules, and any UM decisions already made.
In other words: by the time a claim hits adjudication, UM has already shaped what's payable. A clean claim against a denied authorization still gets denied. That's why fixing claims can't fix UM problems—UM problems have to be fixed at the point UM happens.
For RCM teams, the practical implication is that traditional claims-focused fixes (better coding, faster billing, cleaner submissions) only solve part of the problem. The other part requires upstream changes: stronger eligibility verification, prior auth tracking, concurrent documentation, and appeals workflows.
Is Utilization Management the Same as Prior Authorization?
No, utilization management is not the same as prior authorization.
Prior authorization is one tool inside utilization management—the most visible, most discussed one. UM is the broader program that also includes step therapy, predetermination, concurrent review, and retrospective review.
For providers, focusing only on prior authorization misses the concurrent and retrospective denials that often hit harder. Concurrent reviews can downgrade days mid-stay. Retrospective audits can claw back payment months after care. Both are UM, and neither is prior auth.
The Difference Between Utilization Management and Case Management
Utilization management and case management both fall under the broader care management umbrella—but they do different work, as shown in the table below:
The two disciplines work most effectively when they share information.
Example:
When a case manager spots a complex discharge that's at risk of denial without strong documentation, the UM nurse can adjust the concurrent review submission to head it off. Or when a UM nurse flags a denied day, the case manager rebuilds the discharge plan around the new coverage reality.
2026 Regulatory Changes for Utilization Management in Healthcare
Utilization management has been one of the most actively regulated areas in healthcare over the past two years.
In recent times, three regulatory shifts matter the most:
1. CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F)
Finalized in January 2024, the CMS Interoperability and Prior Authorization Final Rule applies to most government-program payers—Medicare Advantage, Medicaid managed care and fee-for-service, CHIP, and ACA Marketplace QHPs.
Operational requirements take effect January 1, 2026; electronic API requirements follow January 1, 2027. The rule introduces three major changes:
- Faster decisions: Standard prior authorization decisions must be issued within 7 calendar days (down from up to 14), and expedited decisions within 72 hours.
- Transparency requirements: Payers must publicly report PA metrics—volumes, decision times, approval and denial rates—and provide specific reasons for each denial electronically.
- Electronic PA APIs: FHIR-based APIs replace fax submissions and payer-portal logins, allowing providers to submit requests, retrieve documentation requirements, and receive decisions through standardized digital workflows.
CMS estimates the rule will save approximately $15 billion in administrative costs over 10 years.
2. CY 2024 Medicare Advantage Final Rule (CMS-4201-F)
Effective in plan year 2024, the Medicare Advantage Final Rule applies to all Medicare Advantage plans. It introduces three structural changes:
- Mandatory UM Committee. Every MA plan must now have a committee that reviews its UM policies annually to ensure they align with Traditional Medicare coverage rules.
- 90-day continuity of care for new enrollees. When a member switches to a new MA plan, the new plan must honor in-progress treatment authorizations for 90 days.
- Alignment with Traditional Medicare coverage. MA plans can no longer apply stricter coverage criteria than Medicare's national coverage determinations (NCDs) or local coverage determinations (LCDs)—the rules that define what Traditional Medicare will pay for in specific clinical situations.
Together, these changes narrow the coverage gap between MA and Traditional Medicare and add accountability around how MA plans set UM policies.
3. State Legislation and AI Guardrails
State and federal action around utilization management in 2024–2025 fell into three threads:
- State PA reform laws (2024): Ten states passed prior authorization reform legislation in 2024, according to AMA tracking. Common provisions include gold-card programs, faster decision timelines, and public reporting of PA metrics.
- California's AI law (effective January 1, 2025): Senate Bill 1120 (the Physicians Make Decisions Act) requires a licensed physician or qualified healthcare professional to review any denial, delay, or modification of care based on medical necessity—meaning AI tools cannot make those decisions alone.
- Federal AI guardrails (status: not finalized): CMS proposed AI guardrails for MA prior authorization in November 2024 (CMS-4208-P). When the final rule was released in April 2025, those AI provisions had been dropped. CMS may revisit them in future rulemaking.
For RCM leaders, federal AI guardrails are uncertain, but state-level rules and CMS-0057-F's tightened timelines are firmly on the calendar.
Challenges Health Systems Face With Utilization Management
For most hospitals, UM has become one of the largest sources of administrative friction. AMA data shows practices spend roughly 13 hours per physician per week on prior authorization alone—and PA is just one slice of the broader UM workload.
Behind that headline, the operational friction shows up in three predictable patterns.
1. Manual Data Entry Across Fragmented Systems
Staff still rekey information into multiple payer portals, scan and fax documents, and update tracking spreadsheets by hand, even with EHR integrations and advanced AI solutions in the market.
2. Back-and-forth Communication with Payers
Hours on hold, repeated requests for additional documentation, and inconsistent payer status codes consume the workday. Each pended case adds rework hours that don't generate revenue.
3. Limited Real-time Visibility
Without unified dashboards, leaders can't see authorization backlogs, turnaround times, or denial patterns clearly enough to staff appropriately or intervene before cases tip into denial.
The cumulative effect: dedicated prior authorization teams whose primary job is managing UM interactions instead of doing patient-facing work, with denial management cleanup absorbing whatever capacity remains.
That workload doesn't show up on the payer's P&L. It shows up on yours.
How to Manage Utilization Management Better
You can't change the payer's rules. But you can change how predictably your organization moves through them.
Here’s five operational moves separate teams that consume themselves on UM from teams that operationalize it:
1. Hard-wire eligibility and PA detection at scheduling: most authorization-related denials start when services get scheduled before anyone confirms PA requirements. Eligibility verification and pre-auth detection have to happen at scheduling, not at check-in.
2. Standardize documentation for UM-triggered services: build EHR templates and order sets that prompt clinicians to document what payers actually want—duration of symptoms, conservative therapy attempted, severity indicators. Strong documentation is the highest-yield investment for reducing denied authorizations.
3. Track authorizations and denials in one queue: pending, expiring, and denied authorizations need to live in a single work queue with clear ownership, internal turnaround targets shorter than payer SLAs, and priority routing for high-dollar cases.
4. Build CDI workflows that anticipate UM denials: Concurrent and retrospective denials almost always trace back to documentation gaps at the time of admission or service. AI-powered CDI tools surface those gaps in real time, before denials land.
5. Treat payer policy as operational data: payer policies change constantly—new procedures added, criteria tightened, gold-card programs revised. Most organizations track this through ad hoc emails. AI policy monitoring keeps a structured layer with citations and routing into workflows.
How CombineHealth's AI Agents Assist Throughout the Utilization Management Cycle
CombineHealth's AI agents handle three of the most labor-intensive parts of that work:
Eligibility and coverage checks: Mark (AI medical billing solution) runs autonomous eligibility verification and benefits checks across 50+ payer portals in real time, flagging PA requirements before scheduling.
Clinical documentation improvement: Amy (AI medical coding solution) reads encounter notes directly from EMRs and surfaces documentation gaps and undercoded services as they happen—the difference between an approved concurrent review and a denied day.
Payer policy review: Penny (AI policy reviewing solution) monitors CMS manuals, payer policies, LCDs, and NCDs—answering policy questions with page-level citations and catching policy mismatches before claim submission.
Together, they help you reduce preventable UM denials, protect documentation integrity, and stay current with payer rules without adding headcount.
Bring AI to Navigate Utilization Management Better
Teams are working inside a process where the rules belong to someone else, and the workload is structured to make winning hard.
Too much of the day goes into:
- Verifying eligibility one patient at a time
- Tracking down which services need PA
- Re-keying information into payer portals
- Searching for the right policy document
- Defending medical necessity after the fact
This is the work that quietly drains your team's day. Time that could be going into clinical judgment on complex cases, into the appeals that recover real revenue, into the coordination that prevents the next denial.
CombineHealth's AI agents take this off your plate and give that time and efficiency back!
Book a demo to see how it works in practice!
FAQs
1. What is the meaning of utilization management in healthcare?
Utilization management is the set of processes payers use to evaluate whether a service is medically necessary, appropriate, and covered under a member's plan. UM happens in three phases: before care (prior authorization, eligibility), during care (concurrent review), and after care (retrospective review and audits).
2. Is utilization management the same as prior authorization?
No. Prior authorization is one tool within utilization management. UM is the broader program that also includes step therapy, concurrent review, retrospective review, and predetermination.
3. What are the components of utilization management?
The core components are medical necessity criteria (often InterQual or MCG), the three review types (prospective, concurrent, retrospective), payer-side staff (UM nurse, physician advisor, medical director, UM committee), and provider-side workflows for eligibility verification, prior authorization, clinical documentation, and appeals.