What Is a Superbill in Medical Billing and How Does It Work? (A Complete Guide for Billing Teams)
Learn what a superbill is, how it works, and where errors happen. A complete guide for billing teams on generation, payer submission, and AI automation in 2026.
Published on:
March 13, 2026

Key Takeaways:
• A superbill captures every billable service, code, and modifier from a patient encounter and becomes the source document used to generate insurance claims.
• A valid superbill must capture the three core sections: provider information, patient details, and visit information, with medical codes.
• Coding gaps, CPT–ICD mismatches, missing modifiers, and documentation issues in the superbill are common causes of claim denials.
• Superbills move through three operational stages before submission: clinical data extraction, superbill generation, and validation.
• 85% of healthcare leaders are already exploring or adopting generative AI, and among those implementing it, 64% report positive ROI, according to a McKinsey survey.
"Incorrect modifier usage."
"Diagnosis code does not match the services billed."
If you work in medical billing, messages like these are a nightmare—and an expensive one.
A single medical billing error can follow the claim all the way to the payer, come back as a denial, and land back on your team as rework.
When billing teams process hundreds of claims each week, catching every coding gap or error in the documentation becomes nearly impossible. And more often than not, it all traces back to issues like inaccurate or incomplete superbills.
To help you get the superbill right from the start, this guide walks through everything, from what a superbill is and what its elements are, where errors can likely happen, and how AI and automation could be your answer to capturing the right charges every time.
What is a Superbill in Medical Billing?
A superbill is a detailed, itemized document that captures every billable service a provider delivers during a patient encounter. It captures encounter details like medical codes, patient demographics, provider details, and charges for each service.
The provider or their billing team generates the superbill by converting each service—diagnoses, procedures, time spent—into medical codes.
A superbill is often referred to as an encounter form, charge slip, fee ticket, or routing slip.
Why Is a Superbill Important?
A superbill serves as the record of a patient encounter that billing teams use to ensure providers are accurately reimbursed for the services delivered.
But superbills are not submitted as is to insurers. Billing teams convert them into electronic claims—the standardized format payers use to process reimbursements—and submit them through the billing system.
If the superbill contains missing information, incorrect codes, or mismatched documentation, those errors carry forward into the claim.
Even small issues, such as incorrect modifiers, diagnosis-procedure mismatches, or missing provider identifiers, can cause claims to fail validation or be rejected later in the process. (We’ll get into these common errors later.)
This is why superbills are the foundation of payment reimbursement in healthcare RCM.
Key Components of a Valid Superbill
A complete medical superbill has three core components for a clean claim process (as shown in the image below):
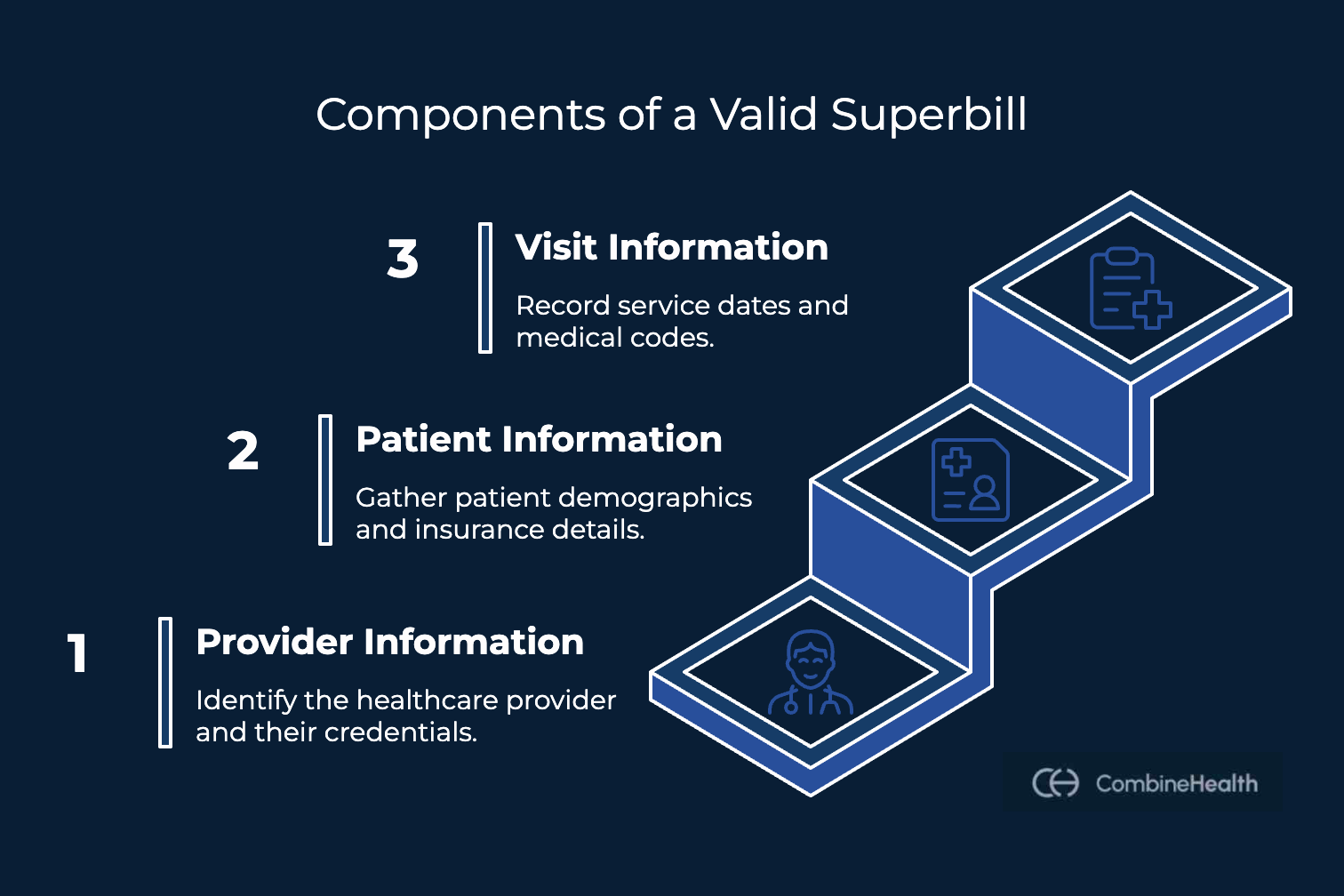
Each component plays a role in ensuring the claim generated from the superbill contains accurate and complete data.
Let's take a deeper look at what each of these contains:
1. Provider information
This section identifies who delivered the care and where it was provided.
It typically includes:
- Provider's full name and credentials
- National Provider Identifier (NPI)—a unique 10-digit number issued by CMS all payers require for claim processing
- Practice name and address
- Provider phone number and email
- Provider signature (required by many payers)
- Referring provider's name and NPI (if applicable)
The NPI in both cases—provider and referral—is non-negotiable.
A missing or incorrect NPI is one of the most common reasons claims are denied at intake.
2. Patient Information
This section identifies who received the care.
It must include:
- Patient's full name and date of birth
- Patient's address and phone number
- Insurance plan name and member ID
- Group number and insurance company contact information
- Policyholder information (if the patient isn't the primary insured)
- The patient's signature authorizing the release of medical information
Errors in patient demographic or insurance data can cause claims to fail eligibility checks before they reach the payer.
3. Visit Information and Medical Codes
This is where the encounter gets converted into billable medical codes and where most of the complexity lives.
It must include:
- Date(s) of service
- CPT Codes–Five-digit codes maintained by the American Medical Association (AMA) that identify the specific procedure or service performed
- ICD-10 Codes–alphanumeric diagnosis codes from the World Health Organization’s classification system, used to explain the necessity to treat the patient
- Modifiers–two-digit codes that provide additional context about how a service was performed (e.g., Modifier 25 indicates a separate E&M visit happened on the same day as a procedure)
- Units or Minutes (for time-based services like therapy)
- Fee charged for each service
The matching between CPT codes and ICD-10 codes is especially important for reimbursement. The diagnosis must justify the procedure.
If those two don’t align—or if the code combination triggers a NCCI edit—the claim will be denied or downcoded.
How do Superbills Work?
A superbill serves as the bridge between the charge generated for a service and the insurance claim submitted for reimbursement.
Understanding how it moves through the billing workflow helps explain where errors can occur and why validation steps are critical.
Below is a simplified overview of how a superbill typically moves through the claim generation process:
Stage 1: Clinical Data Extraction
After the patient encounter, the billing team pulls relevant data from the EHR—patient demographics, provider details, diagnoses, procedures performed, time spent, and other supporting clinical notes.
The accuracy of this data determines everything that follows.
Stage 2: Medical Coding and Charge Capture
Billing teams then convert the clinical documentation into standardized medical codes and billable charges for claim preparation.
This typically involves assigning:
- CPT procedure codes
- ICD-10 diagnosis codes
- Modifiers
- Units or time values
- Service charges
This is one of the most error-prone stages in the process. The volume of claims combined with the complexity of guidelines for each makes errors almost inevitable—even with the best teams.
Stage 3: Superbill Generation
The billing team generates the superbill by compiling the coded services, patient information, provider information, and associated charges into a single itemized document.
The superbill then serves as the structured summary used to generate the insurance claim.
Stage 4: Coding Review and Validation
Before the claim is created, billing teams review the superbill to ensure the information is accurate and compliant with payer guidelines.
Typical checks include:
- Diagnosis-to-procedure alignment
- Correct modifier usage
- National Correct Coding Initiative (NCCI) edits
- Local Coverage Determination (LCD) guidelines
- Authorization references
- Payer-specific billing rules
When done manually, this is where workflows often slow down and errors slip through undetected, especially at high volumes.
How to Submit a Superbill to the Insurance Payer?
In most healthcare organizations, superbills are not submitted directly to the insurers.
The submission process typically follows these steps:
1. Claim Creation
Billing specialists convert the information captured in the superbill into a structured claim format, typically CMS-1500 for professional services or UB-04 for institutional billing.
2. Claim Scrubbing and Validation
Billing teams perform a final claim scrubbing process to make sure the information is accurate and compliant with payer requirements.
3. Clearinghouse Submission
Billing teams submit the prepared claim through a clearinghouse, which validates the claim against HIPAA standards and payer-specific requirements before routing it to the insurer.
If the claim fails clearinghouse validation, the clearinghouse returns it to the billing team for correction and resubmission.
Since the superbill provides the underlying data for the claim, any undetected errors will result in denials and delayed reimbursements.
Common Superbill Errors and What They Cost You
Even with structured workflows in place, errors can still occur during the generation and claim preparation stages.
The scale of billing inaccuracies across healthcare shows how common these issues are: CMS released an improper payment report for FY2025 that puts Medicare FFS improper payments at $28.83 billion, with insufficient provider documentation cited as the primary driver.
This documentation gap often results in an incorrect superbill—downstream in the billing process.
Below are some of the most common superbill errors that contribute to these billing inaccuracies:
Recommended reading: Denial management playbook for RCM leaders
These common errors (and more) occur repeatedly across high-volume billing scenarios.
The good news is that these problems are systematic and recurring across different claim scenarios—which is exactly what makes them solvable with the right technology.
How AI is Transforming Medical Billing Workflows
Traditional medical billing workflows rely heavily on manual steps—from generating the superbills to validating codes and submitting claims.
At high volumes, manual touchpoints almost inevitably lead to errors, denials, and rework that cost billing teams time and revenue.
The healthcare industry is already moving to fix this by deploying AI solutions across RCM workflows.
CombineHealth's Mark (AI medical biller) is part of this shift, purpose-built for medical billing teams.
How CombineHealth’s Mark AI Automates Your Superbill Workflow
Mark integrates directly with EHR systems and automates the entire superbill-to-clearinghouse workflow—eliminating the manual touchpoints where errors typically occur.
Mark handles:
- Superbill generation within existing systems
- Code validation against payer policies, NCCI edits, and LCD guidelines
- Modifier application and correct code sequencing
- Claim preparation and clearinghouse submission
Mark is fully compliant with HIPAA standards, payer rules, and coding guidelines. This ensures every claim that leaves your system is clean and submission-ready.
Bring AI Into Your Superbill Workflow
Manual superbill workflows were built for a different era of billing. Today, the volume is higher, the payer rules are more complex, and the margin for error is smaller.
AI medical billing agents like Mark are built for this environment. They automate the steps where errors happen and get clean claims to the clearinghouse faster.
Book a Demo to see how Mark helps your billing team generate cleaner claims and reduce denials.
FAQs
1. What is a superbill in medical billing?
A superbill in medical billing is a document that summarizes the services delivered during a patient encounter. It includes diagnosis codes, procedure codes, modifiers, and service charges. Billing teams use this information to generate the insurance claim submitted to payers.
2. What is the difference between a superbill and CMS-1500?
A superbill is an internal document used to record services delivered during a patient encounter. It includes diagnosis codes, procedure codes, modifiers, and charges. A CMS-1500 is the standardized claim form generated using the information found in the superbill and submitted to insurers for reimbursement.
3. What happens when a superbill has incorrect codes?
The impact depends on the type of coding error. A wrong ICD-10 code triggers a medical necessity denial. A CPT/ICD-10 mismatch gets the claim denied outright. A missing modifier leads to bundling and partial payment. Every error triggers a rework cycle that costs your team time and pushes out your reimbursement timeline.
4. How do NCCI edits affect superbill submission?
NCCI edits are CMS bundling rules that flag procedure code combinations that can't be billed together. If your superbill includes a conflicting code combination without the right modifier, the claim gets denied or downcoded at the payer level. Getting code sequencing and modifier application right during superbill generation is what prevents this.
5. Can AI agents generate and submit superbills automatically?
Yes. AI medical billing agents integrate directly with EHR systems and automate superbill generation, validation, modifier application, and claim preparation. Human billers then take the validated claim forward for submission. Mark AI is one such agent, built specifically for medical billing workflows.






